Transurethral resection of the prostate
TURP; Prostate resection - transurethral
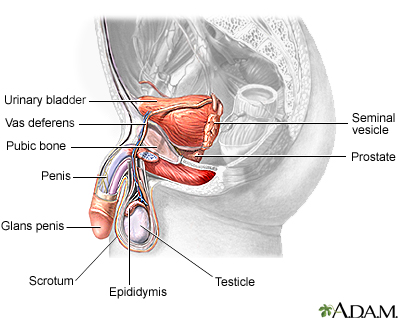
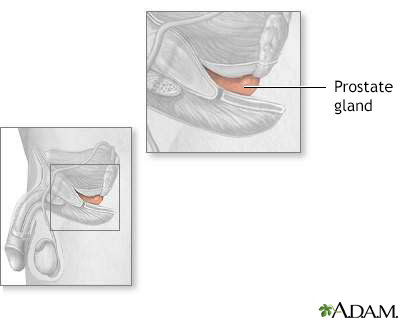
Transurethral resection of the prostate (TURP) is a surgery to remove the inside part of the prostate gland. It is done in order to treat symptoms of an enlarged prostate.
Images
Presentation


Description
The surgery takes about 1 to 2 hours.
You will be given medicine before surgery so you don't feel pain. You may get general anesthesia in which you are asleep and pain-free or spinal anesthesia in which you are awake, but numb from the waist and below.
Your surgeon will insert a scope through the tube that carries urine from your bladder out of the penis. This instrument is called the resectoscope. A special cutting tool is placed through the scope. It is used to remove the inside part of your prostate gland using electricity.
Why the Procedure Is Performed
Your health care provider may recommend this surgery if you have benign prostatic hyperplasia (BPH). The prostate gland often grows larger as men get older. The larger prostate may cause problems with urinating. Removing part of the prostate gland can often make these symptoms better.
TURP may be recommended if you have:
- Difficulty emptying your bladder
- Frequent urinary tract infections
- Bleeding from the prostate
- Bladder stones with prostate enlargement
- Extremely slow urination
- Damage to the kidneys due to an inability to urinate
- Getting up often at night to urinate
- Bladder control issues due to a large prostate
Before you have surgery, your provider will suggest you make changes in how you eat or drink. You may also be asked to try taking medicine. Part of your prostate may need to be removed if these steps do not help. TURP is one of the most common types of prostate surgery. Other procedures are also available.
Your provider will consider the following when deciding on the type of surgery:
- Size of your prostate gland
- Your health
- What type of surgery you may want
- The severity of your symptoms
Risks
Risks for any surgery are:
- Blood clots in the legs that may travel to the lungs
- Breathing problems
- Infection, including in the surgical wound, lungs (pneumonia), bladder or kidney
- Blood loss
- Heart attack or stroke during surgery
- Reactions to medicines
Additional risks are:
- Problems with urine control
- Loss of sperm fertility
- Erection problems
- Passing the semen into the bladder instead of out through the urethra (retrograde ejaculation)
- Urethral stricture (tightening of the urinary outlet from scar tissue)
- Transurethral resection (TUR) syndrome (water buildup during surgery)
- Damage to internal organs and structures
Before the Procedure
You will have many visits with your provider and tests before your surgery. Your visit will include:
- Complete physical exam
- Treating and controlling diabetes, high blood pressure, heart or lung problems, and other conditions
If you are a smoker, you should stop several weeks before the surgery. Your provider can give you tips on how to do this.
Always tell your provider what medicines, vitamins, and other supplements you are taking, even ones you bought without a prescription.
During the weeks before your surgery:
- You may be asked to stop taking medicines that can thin your blood, such as aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), vitamin E, clopidogrel (Plavix), warfarin (Coumadin), apixaban (Eliquis), and others.
- Ask your surgeon which medicines you should still take on the day of your surgery.
On the day of your surgery:
- Do not eat or drink anything after midnight the night before your surgery.
- Take the medicines you have been told to take with a small sip of water.
- You will be told when to arrive at the hospital.
After the Procedure
You will most often stay in the hospital for 1 to 3 days. In some cases, you may be allowed to go home the same day.
After surgery, you will have a small tube, called a Foley catheter, in your bladder to remove urine. Your bladder may be flushed with fluids (irrigated) to keep it clear of clots. The urine will look bloody at first. In most cases, the blood goes away within a few days. Blood can also seep around the catheter. A special solution may be used to flush out the catheter and keep it from getting clogged with blood. The catheter will be removed within 1 to 3 days for most people.
You will be able to go back to eating a normal diet right away.
Your health care team will:
- Help you change positions in bed.
- Teach you exercises to keep blood flowing.
- Teach you how to perform coughing and deep breathing techniques. You should do these every 3 to 4 hours.
- Tell you how to care for yourself after your procedure.
You may need to wear tight stockings and use a breathing device to keep your lungs clear.
You may be given medicine to relieve bladder spasms.
Outlook (Prognosis)
TURP relieves symptoms of an enlarged prostate most of the time. You may have burning with urination, blood in your urine, frequent urination, and need to urgently urinate. This usually resolves after a little bit of time.
Related Information
Enlarged prostateProstate cancer
Frequent or urgent urination
Urinating more at night
Urinary catheters
Bladder stones
Hydronephrosis of one kidney
Neurogenic bladder
Prostate resection - minimally invasive
Simple prostatectomy
Bathroom safety for adults
Surgical wound care - open
Preventing falls
Indwelling catheter care
Kegel exercises - self-care
Transurethral resection of the prostate - discharge
Enlarged prostate - what to ask your doctor
References
Han M, Partin AW. Simple prostatectomy: open and robotic-assisted laparoscopic approaches. In: Partin AW, Domochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 147.
Milam DF. Transurethral resection and transurethral incision of the prostate. In: Smith JA Jr, Howards SS, Preminger GM, Dmochowski RR, eds. Hinman's Atlas of Urologic Surgery. 4th ed. Philadelphia, PA: Elsevier; 2019:chap 67.
Parsons JK, Dahm P, Kohler TS, Lerner LB, Wilt TJ. Surgical management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA Guideline Amendment 2020. J Urol. 2020;204(3):799-804. PMID: 32698710 pubmed.ncbi.nlm.nih.gov/32698710/.
Roehrborn CG, Strand DW. Benign prostatic hyperplasia: etiology, pathophysiology, epidemiology, and natural history. In: Partin AW, Domochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 144.
BACK TO TOPReview Date: 7/1/2023
Reviewed By: Kelly L. Stratton, MD, FACS, Associate Professor, Department of Urology, University of Oklahoma Health Sciences Center, Oklahoma City, OK. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

Health Content Provider
06/01/2025
|
A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complied with the HONcode standard for trustworthy health information from 1995 to 2022, after which HON (Health On the Net, a not-for-profit organization that promoted transparent and reliable health information online) was discontinued. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.