Bronchiolitis
Respiratory syncytial virus - bronchiolitis; Flu - bronchiolitis; Wheezing - bronchiolitis
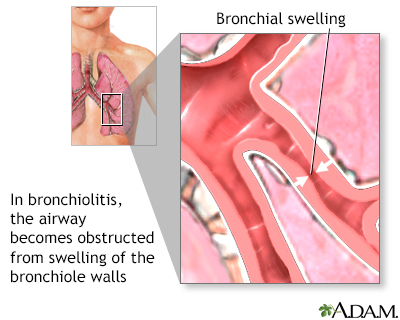
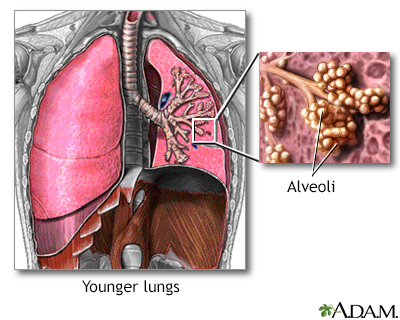
Bronchiolitis is swelling and mucus buildup in the smallest air passages in the lungs (bronchioles). It is usually due to a viral infection.
Images
I Would Like to Learn About:
Causes
Bronchiolitis usually affects children under the age of 2, with a peak age of 3 to 6 months. It is a common, and sometimes severe illness. Respiratory syncytial virus (RSV) is the most common cause. More than half of all infants are exposed to this virus by their first birthday.
Other viruses that can cause bronchiolitis include:
- Adenovirus
- Influenza
- Parainfluenza
The virus is spread to infants by coming into direct contact with nose and throat fluids of someone who has the illness. This can happen when another child or an adult who has a virus:
- Sneezes or coughs nearby and tiny droplets in the air are then breathed in by the infant
- Touches toys or other objects that are then touched by the infant
Bronchiolitis occurs more often in the fall and winter than other times of the year. It is a very common reason for infants to be hospitalized during winter and early spring.
Risk factors of bronchiolitis include:
- Being around cigarette smoke
- Being younger than 6 months old
- Living in crowded conditions
- Not being breastfed
- Being born before 37 weeks of pregnancy
Symptoms
Some children have few or mild symptoms.
Bronchiolitis begins as a mild upper respiratory infection. Within 2 to 3 days, the child develops more breathing problems, including wheezing and a cough.
Symptoms include:
- Bluish skin due to lack of oxygen (cyanosis) - emergency treatment is needed
- Breathing difficulty including wheezing and shortness of breath
- Cough
- Fatigue
- Fever
- Muscles around the ribs sink in as the child tries to breathe in (called intercostal retractions)
- Infant's nostrils get wide when breathing
- Rapid breathing (tachypnea)
Exams and Tests
Your health care provider will perform a physical exam. Wheezing and crackling sounds may be heard through the stethoscope.
Most of the time, bronchiolitis can be diagnosed based on the symptoms and the exam.
Tests that may be done include:
- Blood gases
- Chest x-ray
- Culture of a sample of nasal fluid to determine the virus causing the disease
Treatment
The main focus of treatment is to relieve symptoms, such as difficulty breathing and wheezing. Some children may need to stay in the hospital if their breathing problems do not improve after being observed in the clinic or emergency room.
Antibiotics do not work against viral infections. Medicines that treat viruses may be used to treat very ill children.
At home, measures to relieve symptoms can be used. For example:
- Have your child drink plenty of fluids. Breast milk or formula is fine for children younger than 12 months. Electrolyte drinks, such as Pedialyte, are also OK for infants.
- Have your child breathe moist (wet) air to help loosen sticky mucus. Use a humidifier to moisten the air.
- Give your child saline nose drops. Then use a nasal suction bulb to help relieve a stuffy nose.
- Be sure your child gets plenty of rest.
Do not allow anyone to smoke in the house, car, or anywhere near your child. Children who are having trouble breathing may need to stay in the hospital. There, treatment may include oxygen therapy and fluids given through a vein (IV).
Outlook (Prognosis)
Breathing often gets better by the third day and symptoms mostly clear within a week. In rare cases, pneumonia or more severe breathing problems develop.
Some children may have problems with wheezing or asthma as they get older.
When to Contact a Medical Professional
Contact your provider right away or go to the emergency room if your child:
- Becomes extremely tired
- Has bluish color in the skin, nails, or lips
- Starts breathing very fast
- Has a cold that suddenly worsens
- Has difficulty breathing
- Has nostril flaring or chest retractions when trying to breathe
Prevention
Most cases of bronchiolitis cannot be prevented because the viruses that cause the infection are common in the environment. Careful hand washing, especially around infants, can help prevent the spread of viruses.
A medicine called palivizumab (Synagis) that boosts the immune system may be recommended for certain children. Your child's provider will let you know if this medicine is right for your child.
Related Information
Respiratory syncytial virus (RSV)Hyperventilation
Community-acquired pneumonia in adults
Using oxygen at home - what to ask your doctor
Bronchiolitis - discharge
Using oxygen at home
Oxygen safety
Postural drainage
How to breathe when you are short of breath
References
House SA, Ralston SL. Wheezing, bronchiolitis, and bronchitis. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 418.
Ralston SL, Lieberthal AS; American Academy of Pediatrics, et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):e1474-e1502. PMID: 25349312 pubmed.ncbi.nlm.nih.gov/25349312/.
Walsh EE, Englund JA. Respiratory syncytial virus. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 158.
BACK TO TOPReview Date: 8/5/2023
Reviewed By: Neil K. Kaneshiro, MD, MHA, Clinical Professor of Pediatrics, University of Washington School of Medicine, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

Health Content Provider
06/01/2025
|
A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complied with the HONcode standard for trustworthy health information from 1995 to 2022, after which HON (Health On the Net, a not-for-profit organization that promoted transparent and reliable health information online) was discontinued. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.