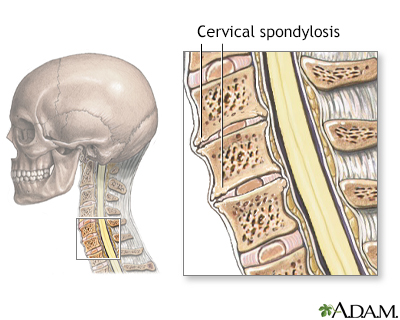
Cervical spondylosis
Cervical osteoarthritis; Arthritis - neck; Neck arthritis; Chronic neck pain; Degenerative disk disease
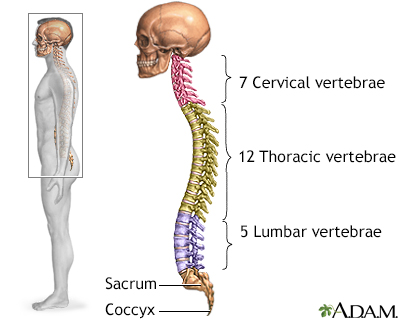
Cervical spondylosis is a disorder in which there is wear on the cartilage (disks) and bones of the neck (cervical vertebrae). It is a common cause of chronic neck pain.
Images
I Would Like to Learn About:
Causes
Cervical spondylosis is caused by aging and chronic wear on the cervical spine. This includes the disks or cushions between the neck vertebrae and the joints between the bones of the cervical spine. There may be abnormal growths or spurs on the bones of the spine (vertebrae).
Over time, these changes can press down on (compress) one or more of the nerve roots. In advanced cases, the spinal cord becomes involved. This can affect your arms, legs, and balance.
Everyday wear and tear may start these changes. People who are very active at work or in sports may be more likely to have them.
The major risk factor is aging. By age 60, most people show signs of cervical spondylosis on x-ray. Other factors that can make someone more likely to develop spondylosis are:
- Being overweight and not exercising
- Having a job that requires heavy lifting or a lot of bending and twisting
- Past neck injury (often several years before)
- Past spine surgery
- Ruptured or slipped disk
- Severe arthritis
- Previous surgery on the neck
Symptoms
Symptoms often develop slowly over time. But they may start or get worse suddenly. The pain may be mild, or it can be deep and so severe that you are unable to move.
You may feel the pain over the shoulder blade. It may spread to the upper arm, forearm, or fingers (in rare cases).
The pain may get worse:
- After standing or sitting
- At night
- When you sneeze, cough, or laugh
- When you bend the neck backward or twist your neck or walk more than a few yards (meters)
You may also have weakness in certain muscles. Sometimes, you may not notice it until your health care provider examines you. In other cases, you will notice that you have a hard time lifting your arm, squeezing tightly with one of your hands, clumsiness of your hand, or other problems.
Other common symptoms are:
- Neck stiffness that gets worse over time
- Numbness or abnormal sensations in the shoulders or arms
- Headaches, especially in the back of the head
- Pain on the inside of the shoulder blade and shoulder pain
Less common symptoms are:
- Loss of balance
- Pain or numbness in the legs
- Loss of control over the bladder or bowels (if there is pressure on the spinal cord)
Exams and Tests
A physical exam may show that you have trouble moving your head toward your shoulder and rotating your head.
Your provider may ask you to bend your head forward and to each side while putting slight downward pressure on the top of your head. Increased pain or numbness during this test is usually a sign that there is pressure on a nerve in your spine.
Weakness of your shoulders and arms or loss of feeling can be signs of damage to certain nerve roots or to the spinal cord.
A spine or neck x-ray may be done to look for arthritis or other changes in your spine.
MRI or CT scans of the neck are done when you have:
- Severe neck or arm pain that does not get better with treatment
- Weakness or numbness in your arms or hands
Electromyography (EMG) and nerve conduction velocity tests may be done to examine nerve root function.
Treatment
Your providers can help you manage your pain so that you can stay active.
- Your provider may refer you for physical therapy. The physical therapist will help you reduce your pain using stretches. The therapist will teach you exercises that make your neck muscles stronger.
- The therapist can also use neck traction to relieve some of the pressure in your neck.
- You may also see a massage therapist, someone who performs acupuncture, or someone who does spinal manipulation (a chiropractor, osteopathic provider, or physical therapist). Sometimes, a few visits will help with neck pain.
- Cold packs and heat therapy may help your pain during flare-ups.
A type of talk therapy called cognitive behavioral therapy may be helpful if the pain is having a serious impact on your life. This technique helps you better understand your pain and teaches you how to manage it.
Medicines can help your neck pain. Your provider may prescribe nonsteroidal anti-inflammatory medicines (NSAIDs) for long-term pain control. Opioids may be prescribed if the pain is severe and does not respond to NSAIDs.
If the pain does not respond to these treatments, or you have a loss of movement or feeling, surgery is considered. Surgery is done to relieve the pressure on the nerves or spinal cord, and it can involve fusion of part of the neck.
Outlook (Prognosis)
Most people with cervical spondylosis have some long-term symptoms. Most of these symptoms improve with non-surgical treatment and do not need surgery.
Many people with this problem are able to maintain an active life. Some people will have to live with chronic (long-term) pain.
Possible Complications
This condition may lead to the following:
- Inability to hold in feces (fecal incontinence) or urine (urinary incontinence)
- Loss of muscle function or feeling
- Permanent disability (occasionally)
- Poor balance
When to Contact a Medical Professional
Contact your provider if:
- The condition becomes worse
- There are signs of complications
- You develop new symptoms (such as loss of movement or feeling in an area of the body)
- You lose control of your bladder or bowels (call right away)
Related Information
ChronicSpinal injury
Bowel incontinence
References
Boody BS, Goldstein ZH, Sasso R. Pathophysiology of cervical spondylosis, radiculopathy, and myelopathy. In: Steinmetz, MP, Berven SH, Benzel EC, eds. Benzel's Spine Surgery. 5th ed. Philadelphia, PA: Elsevier; 2022:chap 29.
Fast A, Dudkiewicz I. Cervical degenerative disease. In: Frontera WR, Silver JK, Rizzo TD, Jr., eds. Essentials of Physical Medicine and Rehabilitation. 4th ed. Philadelphia, PA: Elsevier; 2019:chap 3.
Ronthal M. Arm and neck pain. In: Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 32.
BACK TO TOPReview Date: 4/24/2023
Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

Health Content Provider
06/01/2025
|
A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complied with the HONcode standard for trustworthy health information from 1995 to 2022, after which HON (Health On the Net, a not-for-profit organization that promoted transparent and reliable health information online) was discontinued. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.