Ileostomy - discharge
Standard ileostomy - discharge; Brooke ileostomy - discharge; Continent ileostomy - discharge; Abdominal pouch - discharge; End ileostomy - discharge; Ostomy - discharge; Crohn's disease - ileostomy discharge; Inflammatory bowel disease - ileostomy discharge; Regional enteritis - ileostomy discharge; Ileitis - ileostomy discharge; Granulomatous ileocolitis - ileostomy discharge; IBD - ileostomy discharge; Ulcerative colitis - ileostomy discharge
You had an injury or disease in your digestive system and needed an operation called an ileostomy. The operation changed the way your body gets rid of waste (feces).
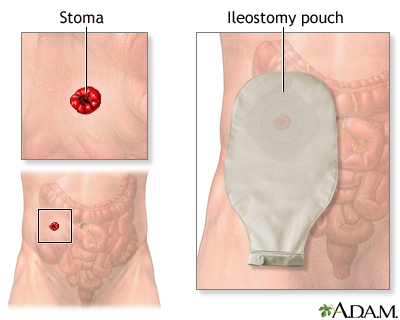
Now you have an opening called a stoma in your belly. Waste will pass through the stoma into a pouch that collects it. You will need to take care of the stoma and empty the pouch many times a day.
Images
What to Expect at Home
Your stoma is made from the lining of your intestine. It will be pink or red, moist, and a little shiny.
Stool that comes from your ileostomy is thin or thick liquid, or it may be pasty. It is not solid like the stool that comes from your colon. Foods you eat, medicines you take, and other things may change how thin or thick your stool is.
Some amount of gas is normal.
You will need to empty the pouch 5 to 8 times a day.
Self-care
Ask your health care provider what you should be eating when you are discharged from the hospital. You may be asked to follow a low-residue diet.
Talk with your provider if you have diabetes, heart disease, or any other condition, and you need to eat or avoid certain foods.
You may take a bath or a shower as air, soap, and water will not hurt your stoma and water will not go into the stoma. It is OK to do this with or without your pouch on.
Medicines:
- Liquid medicines may work better than solid ones. Take these when they are available.
- Some medicines have a special (enteric) coating. Your body will not absorb these well. Ask your provider or pharmacist for other kinds of medicine.
Talk with your provider if you are taking birth control pills. Your body may not absorb them well enough to keep you from getting pregnant.
Emptying and Cleaning Your Pouch
It is best to empty your pouch when it is about one-third to one-half full. It is easier than when it is fuller, and there will be less odor.
To empty your pouch (remember -- stool may keep coming out of the stoma as you do this):
- Wear a clean pair of medical gloves.
- Put some toilet paper in the toilet to keep splashing down. Or, you can flush as you empty the pouch to avoid splashing.
- Sit far back on the seat or on one side of it. You can also stand or stoop over the toilet.
- Hold the bottom of the pouch up.
- Carefully roll the tail of your pouch over the toilet to empty it.
- Clean the outside and inside of the pouch tail with toilet paper.
- Close the pouch at the tail.
Clean and rinse the inside and outside of the pouch.
- Your ostomy nurse may give you a special soap to use.
- Ask your nurse about spraying nonstick oil inside the pouch to keep stool from sticking to it.
You will also need to know about:
Blockages
Chew your food well. This will help keep high-fiber food from blocking your stoma.
Some signs of blockage are sudden cramping in your belly, a swollen stoma, nausea (with or without vomiting), and sudden increase of very watery output.
Drinking hot tea and other liquids may flush any foods that are blocking the stoma.
There will be times when nothing comes out of your ileostomy for a little while. This is normal.
Contact your provider right away if your ileostomy bag stays empty longer than 4 to 6 hours. Your intestine may be blocked.
Do not just take a laxative if this problem happens.
Some foods that may block your stoma are raw pineapple, nuts and seeds, celery, popcorn, corn, dried fruits (such as raisins), mushrooms, chunky relishes, coconut, and some Chinese vegetables.
Tips for when no stool is coming from your stoma:
- Try loosening the opening of the pouch if you think it is too tight.
- Change your position. Try holding your knees up to your chest.
- Take a warm bath or warm shower.
Loose Stools and Increased Output
Some foods will loosen your stools and can increase output after you eat them. If you believe a certain food has caused a change in your stools, do not eat it for a while, and then try again. These foods may make your stools looser:
- Milk, fruit juice, and raw fruits and vegetables
- Prune juice, licorice, large meals, spicy foods, beer, red wine, and chocolate
Some foods will make your stool thicker. Some of these are applesauce, baked potatoes, rice, bread, peanut butter, pudding, and baked apples.
Drink 8 to 10 glasses of fluid a day. Drink more when it is hot or when you have been very active.
If you have diarrhea or your stools are looser or more watery:
- Drink extra fluids with electrolytes (sodium, potassium). Drinks such as Gatorade, PowerAde, or Pedialyte contain electrolytes. Drinking soda, milk, juice, or herbal tea will help you get enough liquids. Avoid caffeine and be aware that some drinks have a high sugar content.
- Try to eat foods that have potassium and sodium every day to keep your potassium and sodium levels from getting too low. Some examples of foods that contain potassium are bananas. Some examples of high-sodium foods are salted snacks.
- Pretzels may help reduce water loss in stool. They also have extra sodium.
- Do not wait to get help. Diarrhea can be dangerous. Contact your provider if it does not go away.
When to Call the Doctor
Contact your provider if:
- Your stoma is swelling and is more than a half inch (1 centimeter) larger than normal.
- Your stoma is pulling in, below the skin level.
- Your stoma is bleeding more than normal.
- Your stoma has turned purple, black, or white.
- Your stoma is leaking often.
- Your stoma does not seem to fit as well as it did before.
- You have a skin rash, or the skin around your stoma is raw.
- You have a discharge from the stoma that smells bad.
- Your skin around your stoma is pushing out.
- You have any kind of sore on the skin around your stoma.
- You have any signs of being dehydrated (there is not enough water in your body). Some signs are dry mouth, urinating less often, and feeling lightheaded or weak.
- You have diarrhea that is not going away.
Related Information
Intestinal obstruction repairLarge bowel resection
Small bowel resection
Ileostomy
Total abdominal colectomy
Total proctocolectomy and ileal-anal pouch
Total proctocolectomy with ileostomy
Crohn disease
Ulcerative colitis
Colorectal cancer
Ileostomy and your child
Ileostomy and your diet
Ileostomy - caring for your stoma
Types of ileostomy
Living with your ileostomy
Small bowel resection - discharge
Total colectomy or proctocolectomy - discharge
Bland diet
Ileostomy - changing your pouch
Crohn disease - discharge
Low-fiber diet
Ulcerative colitis - discharge
Ileostomy - what to ask your doctor
References
American Cancer Society website. What is an ileostomy? www.cancer.org/cancer/managing-cancer/treatment-types/surgery/ostomies/ileostomy/what-is-ileostomy.html. Updated October 16, 2019. Accessed October 18, 2024.
Galandiuk S, Netz U, Morpurgo E, Tosato SM, Abu-Freha N, Ellis CT. Colon and rectum. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. Philadelphia, PA: Elsevier; 2022:chap 52.
Raza A, Araghizadeh F. Ileostomies, colostomies, pouches, and anastomoses. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 117.
BACK TO TOPReview Date: 8/12/2024
Reviewed By: Jenifer K. Lehrer, MD, Gastroenterologist, Philadelphia, PA. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

Health Content Provider
06/01/2025
|
A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complied with the HONcode standard for trustworthy health information from 1995 to 2022, after which HON (Health On the Net, a not-for-profit organization that promoted transparent and reliable health information online) was discontinued. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.