Total abdominal colectomy
Ileorectal anastomosis; Subtotal colectomy
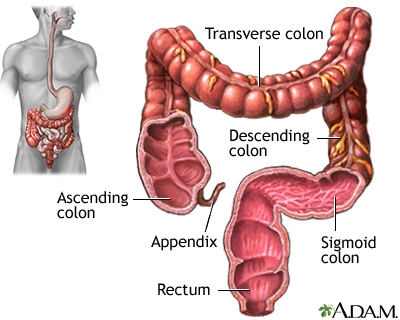
Total abdominal colectomy is the removal of the large intestine from the lowest part of the small intestine (ileum) to the rectum. After it is removed, the end of the small intestine is sewn to the rectum.
Images
I Would Like to Learn About:
Description
You will receive general anesthesia before your surgery. You will be asleep and unable to feel pain.
During the surgery:
- Your surgeon will make a surgical cut in your belly.
- Your surgeon will remove your large intestine. Your rectum and anus will be left in place.
- Your surgeon will connect the end of your small intestine to your rectum.
- Your abdomen will be closed, and your skin from the incision may be left open or closed.
Today, some surgeons perform this operation using a camera that is part of an instrument called a laparoscope. The surgery is done with a few small surgical cuts, and sometimes a larger cut so that the surgeon can also work by hand. The advantages of this surgery, which is called laparoscopy, are a faster recovery, less pain, and only a few small cuts.
Why the Procedure Is Performed
The procedure is done for people who have:
- Crohn disease that has not spread to the rectum or the anus
- Some colon cancer tumors, when the rectum is not affected
- Severe constipation, called colonic inertia
- Severe bleeding of the lower gastrointestinal (GI) tract
- Poor blood supply to the colon, known as colonic ischemia
Risks
Total abdominal colectomy is most often safe. Your risk depends on your general overall health. Ask your surgeon about these possible complications.
Risks of anesthesia and surgery in general are:
- Reactions to medicines
- Breathing problems
- Bleeding, blood clots
- Infection
Risks of having this surgery are:
- Bleeding inside your belly.
- Damage to nearby organs in the body.
- Scar tissue may form in the belly and cause a blockage of the small intestine (this scar tissue is often called adhesions).
- Leakage of stool from the connection between the small intestine and the rectum. This can cause an infection or abscess. It can also turn into a fistula if the stool comes out of an opening in the skin.
- Scarring of the connection between the small intestine and the rectum. This can cause a blockage of the intestine.
- Wound breaking open.
- Wound infection.
- Hernia from the incision
Before the Procedure
Always tell your health care providers what medicines you are taking, even medicines, supplements, or herbs you bought without a prescription. Ask which medicines you should still take on the day of your surgery.
Before you have surgery, talk with your surgeon about the following things:
- Intimacy and sexuality
- Pregnancy
- Sports
- Work
During the 2 weeks before your surgery:
- Before surgery, you may be asked to stop taking medicines that make it harder for your blood to clot. These include aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), and others.
- Ask which medicines you should still take on the day of your surgery.
- If you smoke, you need to stop before operation. Ask your provider for help.
- Always let your provider know about any cold, flu, fever, herpes breakout, or other illnesses you may have before your surgery.
The day before your surgery:
- Follow your surgeon's instructions about what to eat and drink. You may be asked to drink only clear liquids, such as broth, clear juice, and water at some point during the day.
- You will be told when to stop eating and drinking. You may be asked to stop eating solid food after midnight, but you might be able to have clear liquids up until 2 hours before surgery.
- Your surgeon may ask you to use enemas or laxatives to clear out your intestines. You will get instructions on how to use them.
On the day of your surgery:
- Take the medicines you were told to take with a small sip of water.
- You will be told when to arrive at the hospital.
After the Procedure
You will be in the hospital for 3 to 7 days in most cases. By the second day, you will probably be able to drink clear liquids. You will slowly be able to add thicker fluids and then soft foods to your diet as your bowels begin to work again.
Outlook (Prognosis)
After this procedure, you can expect to have 4 to 6 bowel movements a day. You may need more surgery and an ileostomy if you have Crohn disease and it spreads to your rectum.
Most people who have this surgery recover fully. They are able to do most of the activities they were doing before their surgery. This includes most sports, travel, gardening, hiking, and other outdoor activities, and most types of work.
Related Information
IleostomyTotal proctocolectomy and ileal-anal pouch
Total proctocolectomy with ileostomy
Crohn disease
Ulcerative colitis
Ileostomy and your child
Ileostomy and your diet
Ileostomy - caring for your stoma
Types of ileostomy
Ileostomy - discharge
Living with your ileostomy
Bland diet
Ileostomy - changing your pouch
Total colectomy or proctocolectomy - discharge
Low-fiber diet
Ulcerative colitis - discharge
Ileostomy - what to ask your doctor
References
Galandiuk S, Netz U, Morpurgo E, Tosato SM, Abu-Freha N, Ellis CT. Colon and rectum. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. St Louis, MO: Elsevier; 2022:chap 52.
Raza A, Araghizadeh F. Ileostomies, colostomies, pouches, and anastomoses. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 117.
BACK TO TOPReview Date: 9/30/2024
Reviewed By: Jonas DeMuro, MD, Diplomate of the American Board of Surgery with added Qualifications in Surgical Critical Care, Assistant Professor of Surgery, Renaissance School of Medicine, Stony Brook, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

Health Content Provider
06/01/2025
|
A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complied with the HONcode standard for trustworthy health information from 1995 to 2022, after which HON (Health On the Net, a not-for-profit organization that promoted transparent and reliable health information online) was discontinued. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.