Tubal ligation
Sterilization surgery - female; Tubal sterilization; Tube tying; Tying the tubes; Hysteroscopic tubal occlusion procedure; Contraception - tubal ligation; Family planning - tubal ligation
Tubal ligation is surgery to close a woman's fallopian tubes. (It is sometimes called "tying the tubes.") The fallopian tubes connect the ovaries to the uterus. A woman who has this surgery can no longer get pregnant. This means she is "sterile."
Images
Presentation

Description
Tubal ligation is done in a hospital or outpatient surgery facility.
- You may receive general anesthesia. You will be asleep and unable to feel pain.
- Or, you will be awake and given spinal anesthesia. You may also receive medicine to make you sleepy.
- The procedure takes about 30 minutes.
- Your surgeon will make 1 or 2 small surgical cuts in your belly. Most often, they are around the belly button. Gas may be pumped into your belly to expand it. This helps your surgeon see your uterus and fallopian tubes.
- A narrow tube with a tiny camera on the end (laparoscope) is inserted into your belly. Instruments to block off your tubes will be inserted through the laparoscope or through a separate small cut.
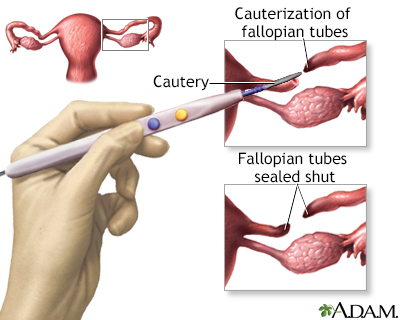
- The tubes are either burned shut (cauterized), clamped off with a small clip or ring (band), or completely removed surgically.
Tubal ligation can also be done right after you have a baby through a small cut in the navel. It can also be done during a C-section.
Why the Procedure Is Performed
Tubal ligation may be recommended for adult women who are sure they do not want to get pregnant in the future. The benefits of this method include a sure way to protect against pregnancy and the lowered risk for ovarian cancer.
Women who are in their 40s or who have a family history of ovarian cancer may want to have the whole tube removed in order to further decrease their risk of later developing ovarian cancer.
However, some women who choose tubal ligation regret the decision later. The younger the woman is, the more likely she will regret having her tubes tied as she gets older.
Tubal ligation is considered a permanent form of birth control. It is NOT recommended as a short-term method or one that can be reversed. However, major surgery can sometimes restore your ability to have a baby. This is called a reversal. More than half of women who have their tubal ligation reversed are able to become pregnant. An alternative to tubal reversal surgery is to have IVF (in vitro fertilization).
Risks
Risks of tubal ligation are:
- Incomplete closing of the tubes, which could make pregnancy still possible. About 1 out of 200 women who have had tubal ligation get pregnant later.
- Increased risk of a tubal (ectopic) pregnancy if pregnancy occurs after a tubal ligation.
- Injury to nearby organs or tissues from surgical instruments.
Before the Procedure
Always tell your health care provider:
- If you are or could be pregnant
- What drugs you are taking, even drugs, herbs, or supplements you bought without a prescription
During the days before your surgery:
- You may be asked to stop taking aspirin, ibuprofen (Advil, Motrin), warfarin (Coumadin), and any other medicines that make it hard for your blood to clot.
- If you smoke, try to stop. Ask your provider for help quitting.
On the day of your surgery:
- You will most often be asked not to drink or eat anything after midnight the night before your surgery, or 8 hours before the time of your surgery.
- Take the drugs your provider told you to take with a small sip of water.
- Your provider will tell you when to arrive at the hospital or clinic.
After the Procedure
You will probably go home the same day you have the procedure. You will need a ride home and will need to have someone with you for the first night if you have general anesthesia.
You will have some tenderness and pain. Your provider will give you a prescription for pain medicine or tell you what over-the-counter pain medicine you can take.
After laparoscopy, many women will have shoulder pain for a few days. This is caused by the gas used in the abdomen to help the surgeon see better during the procedure. You can relieve the gas by lying down.
You can return to most normal activities within a few days, but should avoid heavy lifting for 3 weeks.
Outlook (Prognosis)
Most women will have no problems. Tubal ligation is an effective form of birth control. If the procedure is done with laparoscopy or after delivering a baby, you will NOT need to have any further tests to make sure you cannot get pregnant.
Your periods should return to a normal pattern. If you used hormonal birth control or the Mirena IUD before, then your periods will return to your normal pattern after you stop using these methods.
Women who have a tubal ligation have a decreased risk for developing ovarian cancer.
Related Information
Birth control and family planningSterilization surgery - making a decision
Condoms - male
Female condoms
Vaginal sponge and spermicides
Emergency contraception
Tubal ligation - discharge
References
Isley MM. Postpartum care and long-term health considerations. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 8th ed. Philadelphia, PA: Elsevier; 2021:chap 24.
Rivlin K, Davis AR. Contraception and abortion. In: Gershenson DM, Lentz GM, Valea FA, Lobo RA, eds. Comprehensive Gynecology. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 13.
BACK TO TOPReview Date: 3/31/2024
Reviewed By: LaQuita Martinez, MD, Department of Obstetrics and Gynecology, Emory Johns Creek Hospital, Alpharetta, GA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

Health Content Provider
06/01/2025
|
A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complied with the HONcode standard for trustworthy health information from 1995 to 2022, after which HON (Health On the Net, a not-for-profit organization that promoted transparent and reliable health information online) was discontinued. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- 2025 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.