

Newborn jaundice - discharge
Jaundice of the newborn - discharge; Neonatal hyperbilirubinemia - discharge; Breastfeeding jaundice - discharge; Physiologic jaundice - dischargeYour baby has been treated in the hospital for newborn jaundice. This article tells you what you need to know when your baby comes home.

- When Your Child Was in the Hospital
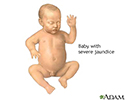
Your baby has newborn jaundice. This common condition is caused by high levels of bilirubin in the blood. Your child's skin and sclera (whites of their eyes) will look yellow.
Some newborns need to be treated before they leave the hospital. Others may need to go back to the hospital when they are a few days old. Treatment in the hospital most often lasts 1 to 2 days. Your child needs treatment when their bilirubin level is too high or rising too quickly.
To help break down the bilirubin, your child will be placed under bright lights (phototherapy) in a warm, enclosed bed. The infant will wear only a diaper and special eye shades. Your baby may have an intravenous (IV) line to give them fluids.
Rarely, your baby may need treatment called a double volume blood exchange transfusion. This is used when the baby's bilirubin level is very high.
Unless there are other problems, your child will be able to feed (by breast or bottle) normally. Your child should feed every 2 to 2 ½ hours (10 to 12 times a day).
The health care provider may stop phototherapy and send your child home when their bilirubin level is low enough to be safe. Your child's bilirubin level will need to be checked in the provider's office, 24 hours after therapy stops, to make sure the level is not rising again.
Possible side effects of phototherapy are watery diarrhea, dehydration, and skin rash that will go away once the therapy stops.
- What to Expect at Home
If your child did not have jaundice at birth but now has it, you should call your provider. Bilirubin levels are generally the highest when a newborn is 3 to 5 days old.
If the bilirubin level is not too high or not rising quickly, you can do phototherapy at home with a fiber optic blanket, which has tiny bright lights in it. You may also use a bed that shines light up from the mattress. A nurse will come to your home to teach you how to use the blanket or bed and to check on your child.
The nurse will return daily to check your child's:
- Weight
- Intake of breast milk or formula
- Number of wet and poopy (stool) diapers
- Skin, to see how far down (head to toe) the yellow color goes
- Bilirubin level
You must keep the light therapy on your child's skin and feed your child every 2 to 3 hours (10 to 12 times a day). Feeding prevents dehydration and helps bilirubin leave the body.
Therapy will continue until your baby's bilirubin level lowers enough to be safe. Your baby's provider will want to check the level again in 2 to 3 days.
If you are having trouble breastfeeding, contact a breastfeeding nurse specialist.
- When to Call the Doctor
Contact your baby's health care provider if the infant:
- Has a yellow color that goes away, but then returns after treatment stop
- Has a yellow color that lasts for more than 2 to 3 weeks
Also contact your baby's provider if you have concerns, if the jaundice is getting worse, or the baby:
- Is lethargic (hard to wake up), less responsive, or fussy
- Refuses the bottle or breast for more than 2 feedings in a row
- Is losing weight
- Has watery diarrhea
References
Kaplan M, Wong RJ, Burgis JC, Sibley E, Stevenson DK. Neonatal jaundice and liver diseases. In: Martin RJ, Fanaroff AA, Walsh MC, eds. Fanaroff and Martin's Neonatal-Perinatal Medicine. 11th ed. Philadelphia, PA: Elsevier; 2020:chap 91.
Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM. Digestive system disorders. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 123.
Rozance PJ, Wright CJ. The neonate. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 8th ed. Philadelphia, PA: Elsevier; 2021:chap 23.



, life-threatening infection, severe disturbances in body chemistry, toxic effects of drugs, polycythemia. </p>")