C-section
Abdominal delivery; Abdominal birth; Cesarean birth; Pregnancy - cesareanA C-section is the delivery of a baby by making an opening in the mother's lower belly area. It is also called a cesarean delivery.
-
Description
A C-section delivery is done when it is not possible or safe for the mother to deliver the baby through the vagina.
The procedure is most often done while the woman is awake. The body is numbed from the chest to the feet using epidural or spinal anesthesia.
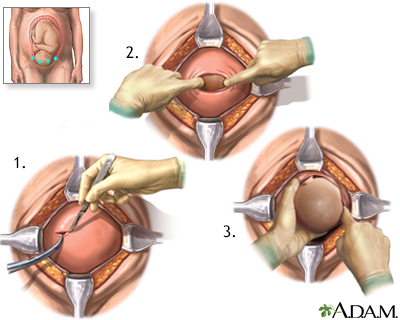
/1. The surgeon makes a cut across the belly just above the pubic area.
2. The womb (uterus) and amniotic sac are opened.
3. The baby is delivered through this opening.
The health care team clears fluids from the baby's mouth and nose. The umbilical cord is cut. The health care provider will make sure that the infant's breathing is normal and other vital signs are stable.
The mother is awake during the procedure so she will be able to hear and see her baby. In many cases, the woman is able to have a support person with her during the delivery.
The surgery takes about 1 hour.
-
Why the Procedure Is Performed
There are many reasons why a woman may need to have a C-section instead of a vaginal delivery. The decision will depend on your provider, where you are having the baby, your previous deliveries, and your medical history.
Problems with the baby may include:
- Abnormal heart rate
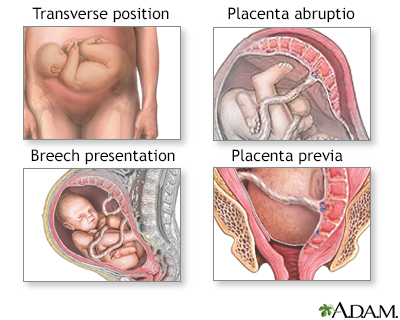
- Abnormal position in the womb, such as crosswise (transverse) or feet-first (breech)
- Developmental problems, such as hydrocephalus or spina bifida
- Multiple pregnancy (twins, triplets, or more)
Health problems in the mother may include:
- Active genital herpes infection
- Large uterine fibroids near the cervix
- HIV infection in the mother
- Past C-section
- Past surgery on the uterus
- Severe illness, such as heart disease, preeclampsia or eclampsia
Problems at the time of labor or delivery may include:
- Baby's head is too large to pass through the birth canal
- Labor that takes too long or stops
- Very large baby
- Infection or fever during labor
Problems with the placenta or umbilical cord may include:
- Placenta covers all or part of the opening to the birth canal (placenta previa)
- Placenta separates from the uterine wall (placenta abruptio)
- Umbilical cord comes through the opening of the birth canal before the baby (umbilical cord prolapse)
/



-
Risks
A C-section is a safe procedure. The rate of serious complications is very low. However, certain risks are higher after C-section than after vaginal delivery. These include:
- Infection of the bladder or uterus
- Injury to the urinary tract
- Higher average blood loss
Most of the time, a blood transfusion is not needed, but risk of transfusion is higher.
A C-section may also cause problems in future pregnancies. This includes a higher risk for:
- Placenta previa
- Placenta growing into the muscle of the uterus and has trouble separating after the baby is born (placenta accreta)
- Uterine rupture
These conditions can lead to severe bleeding (hemorrhage), which may require blood transfusions or removal of the uterus (hysterectomy).
-
After the Procedure
Most women will remain in the hospital for 2 to 3 days after a C-section. Take advantage of the time to bond with your baby, get some rest, and receive some help with breastfeeding and caring for your baby.
Recovery takes longer than it would from a vaginal birth. You should walk around after the C-section to speed recovery. Pain medicines taken by mouth can help ease discomfort.
Recovery after a C-section at home is slower than after a vaginal delivery. You may have bleeding from your vagina for up to 6 weeks. You will need to learn to care for your wound.

-
Outlook (Prognosis)
Most mothers and infants do well after a C-section.
Women who have a C-section may have a vaginal delivery if another pregnancy occurs, depending on:
- The type of C-section done
- Why the C-section was done
Vaginal birth after cesarean (VBAC) delivery is very often successful. Not all hospitals or providers offer the option of VBAC. There is a small risk of uterine rupture, which can harm the mother and the baby. Discuss the benefits and risks of VBAC with your provider.
References
Berghella V, Mackeen AD, Jauniaux ERM. Cesarean delivery. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 19.
Hull AD, Resnik R, Silver RM. Placenta previa and accreta, vasa previa, subchorionic hemorrhage, and abruptio placentae. In: Lockwood CJ, Copel JA, Dugoff L, et al, eds. Creasy and Resnik's Maternal-Fetal Medicine: Principles and Practice. 9th ed. Philadelphia, PA: Elsevier; 2023:chap 43.