



CMV - gastroenteritis/colitis
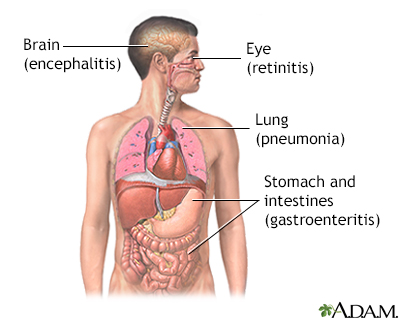
Colitis - cytomegalovirus; Gastroenteritis - cytomegalovirus; Gastrointestinal CMV diseaseCMV gastroenteritis/colitis is inflammation of the stomach or intestine due to infection with cytomegalovirus.
This same virus can also cause:



-
Causes
Cytomegalovirus (CMV) is a herpes-type virus. It is related to the virus that causes chickenpox.
Infection with CMV is very common. It is spread by saliva, urine, respiratory droplets, sexual contact, and blood transfusions. Most people are exposed at some point, but most of the time, the virus produces mild or no symptoms in healthy people.
Serious CMV infections can occur in people with weakened immune systems due to:
- AIDS
- Chemotherapy treatment for cancer
- During or after bone marrow or organ transplant
- Ulcerative colitis or Crohn disease
Rarely, serious CMV infection involving the GI tract has occurred in people with a healthy immune system.




-
Symptoms
Gastrointestinal (GI) CMV disease may affect one area or the entire GI system. Ulcers due to CMV can occur in the esophagus, stomach, small intestine, or colon. These ulcers are associated with symptoms such as:
- Abdominal pain
- Difficulty swallowing or pain with swallowing
- Nausea
- Vomiting
When the intestines are involved, the ulcers may cause:
- Abdominal pain
- Bloody stools
- Diarrhea
- Fever
- Weight loss
More severe infections can result in gastrointestinal bleeding or a hole through the wall of the bowel (perforation).





-
Exams and Tests
Tests that may be done include:
- Barium enema
- Colonoscopy with biopsy
- Upper endoscopy (EGD) with biopsy
- Stool culture or similar stool tests to check for other causes of infection
- Upper GI and small bowel series
Laboratory tests will be done on a sample of tissue taken from your stomach or intestine. The tests, such as a gastric or intestinal tissue culture or biopsy, determine if the virus is in the tissue.
A CMV serology test may be done to look for antibodies to the CMV virus in your blood.
Another blood test that looks for the presence and number of virus particles in the blood can also be done.






-
Treatment
Treatment is meant to control the infection and relieve symptoms.
Medicines to fight the virus (antiviral medicines) are prescribed. The medicines may be given through a vein (IV), and sometimes by mouth, for several weeks. The most commonly used medicines are ganciclovir, valganciclovir, and foscarnet.
In some cases, long-term therapy may be needed. A medicine called CMV hyperimmune globulin may be used when other medicines don't work.
Other medicines may include:
- Medicines to prevent or reduce diarrhea
- Painkillers (analgesics)
Nutritional supplements or nutrition given through a vein (IV) may be used to treat muscle loss due to the disease.
-
Outlook (Prognosis)
In people with a healthy immune system, symptoms go away without treatment in most cases.
Symptoms are more severe in those with a weakened immune system. The outcome depends on how severe the immune system deficiency and the CMV infection are.
People with AIDS may have a worse outcome than those with a weakened immune system due to another reason.
CMV infection typically affects the entire body, even if only (GI) symptoms are present. How well a person does depends on how well the antiviral medicines work.
-
Possible Complications
The medicines used to fight the virus may cause side effects. The type of side effect depends on the specific medicine used. For example, ganciclovir may lower your white blood cell count. Another medicine, foscarnet, may lead to kidney problems.
-
When to Contact a Medical Professional
Contact your health care provider if you have symptoms of CMV gastroenteritis/colitis.
-
Prevention
There is a high risk of CMV infection in people who receive an organ transplant from a CMV-positive donor. Taking the antiviral medicines ganciclovir (Cytovene) and valganciclovir (Valcyte) by mouth before the transplant can lower your chance of getting a new infection or reactivating an old infection.
People with AIDS who are effectively treated with highly active antiretroviral therapy are much less likely to get a CMV infection.
References
Britt WJ. Cytomegalovirus. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 137.
Fleckenstein JM. Approach to the patient with suspected enteric infection. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 262.
Larson AM, Issaka RB, Hockenbery DM. Gastrointestinal and hepatic complications of solid organ and hematopoietic cell transplantation. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 36.
Wilcox CM. Gastrointestinal consequences of infection with human immunodeficiency virus. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 35.