| ||||||||||||||||||||||||||||||||||||||||
Once you arrive at the hospital in labor, there are certain procedures that may be done. Your health and the baby's health will be monitored while you are in labor. In some cases, the doctor may need to assist with the delivery using forceps or vacuum extraction.
Your health care providers will monitor your baby's heart rate. This allows them to check the well-being of the baby while you are in labor. Fetal heart monitoring does not prevent a problem from occurring. But changes in the baby's heart rate can alert the providers that something might be wrong.
Auscultation. The nurse or doctor will listen to the baby's heart at set times during labor. They will listen to the heart rate using either:
External electronic fetal monitoring. In this method:
These two measurements will provide detailed information as to how your baby is doing during labor.
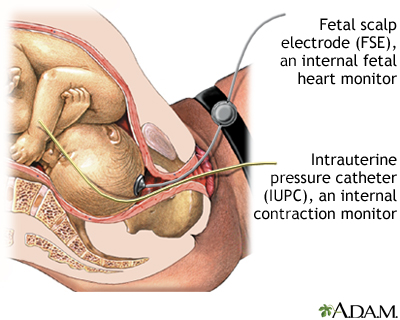
Internal electronic fetal monitoring. An internal monitor can only be used once your "water has broken" and your cervix has dilated enough. A small clip is placed on the baby's scalp to directly monitor the fetal heart rate. The clip is called a fetal scalp electrode (FSE).
Internal contraction monitoring. To gauge the strength of your contractions, a small catheter (Intrauterine pressure catheter or IUPC) is placed in your uterus. Combined with an internal fetal monitor, an IUPC may give a more precise reading of the baby's heart rate and your contractions.
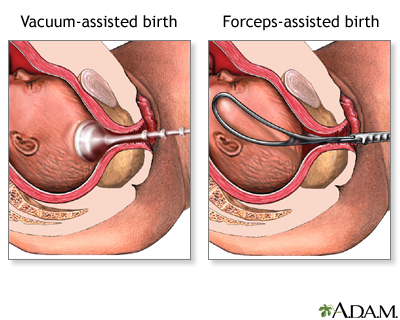
There are times when it is necessary to help the delivery along using forceps or a vacuum extractor. Forceps resemble two large salad spoons, and the doctor uses them to guide the baby's head out of the birth canal. Vacuum extraction uses a soft plastic cup that is applied to the baby's head and stays in place by suction. There is a handle on the cup that allows the doctor to use this to assist with delivery through the birth canal. The choice between using forceps or a vacuum extractor is usually made by the doctor.
These methods are sometimes in these cases:
The second stage of labor can take a long time, and it may be tempting to ask for a little help with a vacuum or forceps. But studies suggest that the safest route, for your bottom and for your baby, is to deliver without a vacuum or forceps. Assisted delivery is associated with more severe tears and more urinary and bowel problems for mom. Moreover, babies delivered with vacuums or forceps may have bump or bruises from their hasty exit through the birth canal. That's why your health care provider will not use forceps or vacuum unless there's a compelling reason to help speed up delivery.
When applied properly, forceps or vacuum deliveries rarely cause any permanent injury to the baby. The forceps' marks on the baby's cheeks usually disappear in a few days. Very rarely, the baby's facial nerves may be temporarily injured. The resulting drooping of facial muscles almost always recovers completely in a matter of weeks. Caput succedaneum is diffuse swelling of the scalp due to molding after prolonged labor. A vacuum delivery may leave a more noticeable caput. Caput usually disappears in 2 to 3 days. In rare cases, the vacuum device can cause bleeding within the brain.
|
Review Date:
8/22/2019 Reviewed By: LaQuita Martinez, MD, Department of Obstetrics and Gynecology, Emory Johns Creek Hospital, Alpharetta, GA. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. |
 All rights reserved.
All rights reserved.


