| ||||||||||||||||||||||||||||||||||||||||
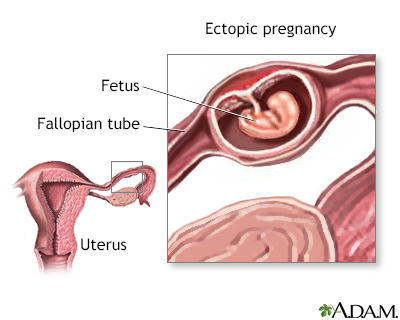
An ectopic pregnancy occurs when the fertilized egg implants in some part of the body other than the uterus. In 95% of all ectopic pregnancies, the egg is implanted in one of the fallopian tubes. In rare cases, these types of pregnancies occur in the ovaries, the abdomen, and in the lower portion of the uterus (cervix). Alternative names are abdominal, cervical, or tubal pregnancy.
If left untreated, an ectopic pregnancy can tear or rupture the fallopian tube, which is not designed to accommodate a growing embryo. An ectopic pregnancy can lead to severe, life-threatening internal bleeding.
Although all women are at risk, most ectopic pregnancies occur in women between the ages of 35 to 44. Ectopic pregnancy is also more prevalent in women whose fallopian tubes have been blocked or damaged due to endometriosis, scarring after tubal surgery, pelvic inflammatory disease (PID), or a previous ectopic pregnancy. Other risk factors include infertility, exposure to several STDs, smoking, and having an IUD in place during conception.
About 2 of every 100 pregnancies are ectopic. Thanks to new techniques for early diagnosis and medical care, they are usually treated by the eighth week of pregnancy, eliminating much of the risk to the mother. Unfortunately, though, since the fetus cannot survive outside of the uterus, the pregnancy cannot survive the treatment.
Immediate medical attention can often save the fallopian tube and improve your chances of remaining fertile in the future. If you are experiencing any or all of these symptoms, please call your health care provider:
If your health care provider suspects an ectopic pregnancy, she will perform a pelvic exam. Next, you will undergo some of the following tests:
Treatment of an ectopic pregnancy usually consists of surgery called laparoscopy. In this procedure, a small incision is made in the lower abdomen, near or in the navel. Your surgeon then inserts a long, thin camera called a laparoscope into the pelvic region. This allows the surgeon to remove the embryo and repair or remove the affected fallopian tube.
Unless the fallopian tube has irreparable damage, it is usually possible to save it. This will improve your chances of a successful pregnancy in the future, though it may also be the site of a future ectopic pregnancy. A follow-up test of your hCG level is performed later to ensure that the entire ectopic pregnancy was removed.
The drug methotrexate is a medical alternative to surgery. An injection of the medication impairs cell growth and usually terminates the pregnancy. You’ll then need to come back for a series of blood tests to make sure the medicine has been effective. If the medicine isn’t working, you may need a second dose of medication. The tube may rupture even after treatment, and you’ll need to have surgery to remove the abnormal pregnancy.
Ectopic pregnancies may be prevented by avoiding conditions that cause scarring or blocking to the fallopian tubes. This includes early diagnosis and adequate treatment of pelvic inflammatory disease (PID), STDs, and the avoidance of smoking.
As always, it's important to talk to your health care provider before planning your pregnancy to ensure the best care possible.
Q: I've been having periodic cramping. Could I have an ectopic pregnancy without even knowing it?
A: Occasional cramping is most likely the result of ligaments stretching as your uterus grows, but an ectopic pregnancy can still cause occasional cramping. Cramping caused by an ectopic pregnancy is usually more constant and sharp, usually occurring in the lower abdomen only. But if the pain is persistent and worse than your normal period cramps, or if you’re unsure, contact your health care provider.
Q: Why have ectopic pregnancies become more common as of late?
A: No one is certain why ectopic pregnancies have become more common. Some medical professionals believe that an increase in pelvic inflammatory disease (PID) is partially responsible.
Q: I've had an ectopic pregnancy before. What are my chances of having a successful pregnancy later?
A: Although the chances of having a successful pregnancy are lowered if you've already had an ectopic pregnancy, you still have a 60% chance of uterine implantation if your fallopian tube has not been removed. Even if one fallopian tube has been removed, your chances are as high as 40%. Women treated with methotrexate have about a 50% chance of a future normal pregnancy. Notably, women who keep their tube at the time of surgery have a higher risk of another ectopic pregnancy (about 15%) than those who have the tube removed (about 10%).
|
Review Date:
12/9/2012 Reviewed By: Irina Burd, MD, PhD, Maternal Fetal Medicine, Johns Hopkins University, Baltimore, MD. Review provided by VeriMed Healthcare Network. |
 All rights reserved.
All rights reserved.


