
Diskectomy
Spinal microdiskectomy; Microdecompression; Laminotomy; Disk removal; Spine surgery - diskectomy; DiscectomyDiskectomy is surgery to remove all or part of the cushion that helps support part of your spinal column. These cushions are called disks, and they separate your spinal bones (vertebrae).
Description
A surgeon may perform disk removal (diskectomy) in these different ways.
- Microdiskectomy: When you have a microdiskectomy, the surgeon does not need to do much surgery on the bones, joints, ligaments, or muscles of your spine.
- Diskectomy in the lower part of your back (lumbar spine) may be part of a larger surgery that also includes a laminectomy, foraminotomy, or spinal fusion.
Laminectomy
Laminectomy is surgery to remove the lamina. This is part of the bone that makes up a vertebra in the spine. Laminectomy may also be done to remove...
Read Article Now Book Mark ArticleForaminotomy
Foraminotomy is surgery that widens the opening (the foramen) in your spine where nerve roots leave your spinal canal. You may have a narrowing of t...
Read Article Now Book Mark ArticleSpinal fusion
Spinal fusion is surgery to permanently join together two or more bones in the spine so there is no movement between them. These bones are called ve...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Diskectomy in your neck (cervical spine) is most often done along with foraminotomy, or fusion.
Microdiskectomy is done in a hospital or outpatient surgical center. You will be given general anesthesia. You will be asleep and pain-free.
- The surgeon makes a small (1 to 1.5-inch, or 2.5 to 3.8-centimeter) incision (cut) on your back and moves the back muscles away from your spine. The surgeon uses a special microscope to see the problem disk or disks and nerves during surgery.
- The nerve root is located and gently moved away.
- The surgeon removes the injured disk tissue and pieces of the disk.
- The back muscles are returned to their normal place.
- The incision is closed with stitches or staples.
- The surgery takes about 1 to 2 hours.
Diskectomy and laminotomy are usually done in the hospital, using general anesthesia (asleep and pain-free).
- The surgeon makes a larger cut on your back over the spine.
- Muscles and tissue are gently moved to expose your spine.
- A small part of the lamina bone (part of the vertebrae that surrounds the spinal column and nerves) is cut away. The opening may be as large as the ligament that runs along your spine.
- A small hole is cut in the disk that is causing your symptoms. Material from inside the disk is removed. Other fragments of the disk may also be removed.
Why the Procedure Is Performed
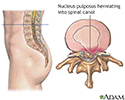
When one of your disks moves out of place (herniates), the soft gel inside pushes through the wall of the disk. The disk may then place pressure on the spinal cord and nerves that are coming out of your spinal column.
Herniates
A herniated (slipped) disk occurs when all or part of a disk is forced through a weakened part of the disk. This may place pressure on nearby nerves...

Many of the symptoms caused by a herniated disk get better or go away over time without surgery. Most people with low back or neck pain, numbness, or even mild weakness are often first treated with anti-inflammatory medicines, physical therapy, and exercise.
Only a few people with a herniated disk need surgery.
Your health care provider may recommend a diskectomy if you have a herniated disk and:
- Leg or arm pain or numbness that is very bad or is not going away, making it hard to do daily tasks
- Severe weakness in muscles of your arm, lower leg or buttocks
- Pain that spreads into your buttocks or legs
If you are having problems with your bowels or bladder, or the pain is so bad that strong pain medicines do not help, you will need to have surgery right away.
Risks
Risks of anesthesia and surgery in general are:
- Reactions to medicines
- Breathing problems
- Bleeding, blood clots, infection
Risks of this surgery are:
- Damage to the nerves that come out of the spine, causing weakness or pain that does not go away.
- Your back pain does not get better, or pain comes back later.
- Pain after surgery, if all the disk fragments are not removed.
- Spinal fluid may leak and cause headaches.
- The disk may bulge out again.
- Your spine may become more unstable and require more surgery.
- Infection that may require antibiotics, a longer hospital stay, or more surgery.
Before the Procedure
Tell your surgeon what medicines you are taking, even medicines, supplements, or herbs you bought without a prescription.
During the days before the surgery:
- Prepare your home for when you come back from the hospital.
- If you are a smoker, you need to stop, ideally 4 weeks before your surgery. Your recovery will be slower and possibly not as good if you continue to smoke. Ask your provider for help.
Smoker, you need to stop
There are many ways to quit smoking. There are also resources to help you. Family members, friends, and co-workers may be supportive. But to be su...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Two weeks before surgery, you may be asked to stop taking medicines that make it harder for your blood to clot. These include aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), and other medicines like these.
- If you have diabetes, heart disease, or other medical problems, your surgeon will ask you to see the providers who treat you for those conditions before your surgery.
Diabetes
Diabetes is a long-term (chronic) disease in which the body cannot regulate the amount of sugar in the blood.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleHeart disease
Coronary heart disease is a narrowing of the blood vessels that supply blood and oxygen to the heart. Coronary heart disease (CHD) is also called co...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Talk with your provider if you have been drinking a lot of alcohol, more than 1 or 2 drinks a day.
- Ask your surgeon which medicines you should still take on the day of the surgery.
- Always let your surgeon know about any cold, flu, fever, herpes breakout, or other illnesses you may have.
- You may want to visit the physical therapist to learn some exercises to do before surgery and to practice using crutches.
On the day of the surgery:
- Follow instructions about when to stop eating and drinking.
- Take the medicines your surgeon told you to take with a small sip of water.
- Bring your cane, walker, or wheelchair if you have one already. Also bring shoes with flat, nonskid soles.
- Follow instructions about when to arrive at the hospital. Arrive on time.
After the Procedure
Your surgeon will ask you to get up and walk around as soon as your anesthesia wears off. Most people go home the day of surgery. Do not drive yourself home.
Follow instructions about how to care for yourself at home.
Care for yourself at home
You were in the hospital for spine surgery. You probably had a problem with one or more disks or spine bones. A disk is a cushion that separates th...

Outlook (Prognosis)
Most people have pain relief and can move better after surgery. Numbness and tingling should get better or disappear. Your pain, numbness, or weakness may not get better or go away if you had nerve damage before surgery, or if you have symptoms caused by other spinal conditions.
Further changes may occur in your spine over time and new symptoms may occur.
Talk with your provider about how to prevent future back problems.
References
Gardocki RJ. Anatomic approaches to the spine. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 37.
Gardocki RJ, Park AL. Degenerative disorders of the thoracic and lumbar spine. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 39.
Ryu WHA, O’Toole JE. Cervical spine and cervicothoracic junction - anterior approach. In: Steinmetz MP, Berven SH, Benzel EC, eds. Benzel's Spine Surgery. 5th ed. Philadelphia, PA: Elsevier; 2022:chap 109.
-
Herniated nucleus pulposus - illustration
Herniated nucleus pulposus is a condition in which part or all of the soft, gelatinous central portion of an intervertebral disk is forced through a weakened part of the disk, resulting in back pain and nerve root irritation.
Herniated nucleus pulposus
illustration
-
Skeletal spine - illustration
The spine is divided into several sections. The cervical vertebrae make up the neck. The thoracic vertebrae comprise the chest section and have ribs attached. The lumbar vertebrae are the remaining vertebrae below the last thoracic bone and the top of the sacrum. The sacral vertebrae are caged within the bones of the pelvis, and the coccyx represents the terminal vertebrae or vestigial tail.
Skeletal spine
illustration
-
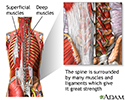
Spine supporting structures - illustration
The spine is surrounded by many muscles and ligaments which give it great strength and flexibility. If these muscles or ligaments become damaged, back pain results.
Spine supporting structures
illustration
-
Cauda equina - illustration
The spinal cord ends in the lumbar area and continues through the vertebral canal as spinal nerves. Because of its resemblance to a horses tail, the collection of these nerves at the end of the spinal cord is called the cauda equina. These nerves send and receive messages to and from the lower limbs and pelvic organs.
Cauda equina
illustration
-
Spinal stenosis - illustration
Spinal stenosis is a narrowing of the lumbar or cervical spinal canal. The narrowing can cause compression on nerve roots resulting in pain or weakness of the legs. Medications or steroid injections are often administered to reduce inflammation. If the pain is persistent and does not respond to these conservative measures, surgery is considered to relieve the pressure on the nerves.
Spinal stenosis
illustration
-
Microdiskectomy - series
Presentation









-
Herniated nucleus pulposus - illustration
Herniated nucleus pulposus is a condition in which part or all of the soft, gelatinous central portion of an intervertebral disk is forced through a weakened part of the disk, resulting in back pain and nerve root irritation.
Herniated nucleus pulposus
illustration
-
Skeletal spine - illustration
The spine is divided into several sections. The cervical vertebrae make up the neck. The thoracic vertebrae comprise the chest section and have ribs attached. The lumbar vertebrae are the remaining vertebrae below the last thoracic bone and the top of the sacrum. The sacral vertebrae are caged within the bones of the pelvis, and the coccyx represents the terminal vertebrae or vestigial tail.
Skeletal spine
illustration
-
Spine supporting structures - illustration
The spine is surrounded by many muscles and ligaments which give it great strength and flexibility. If these muscles or ligaments become damaged, back pain results.
Spine supporting structures
illustration
-
Cauda equina - illustration
The spinal cord ends in the lumbar area and continues through the vertebral canal as spinal nerves. Because of its resemblance to a horses tail, the collection of these nerves at the end of the spinal cord is called the cauda equina. These nerves send and receive messages to and from the lower limbs and pelvic organs.
Cauda equina
illustration
-
Spinal stenosis - illustration
Spinal stenosis is a narrowing of the lumbar or cervical spinal canal. The narrowing can cause compression on nerve roots resulting in pain or weakness of the legs. Medications or steroid injections are often administered to reduce inflammation. If the pain is persistent and does not respond to these conservative measures, surgery is considered to relieve the pressure on the nerves.
Spinal stenosis
illustration
-
Microdiskectomy - series
Presentation
Review Date: 4/24/2023
Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.