
Clubfoot repair
Repair of clubfoot; Posteromedial release; Achilles tendon release; Clubfoot release; Talipes equinovarus - repair; Tibialis anterior tendon transferClubfoot repair is surgery to correct a birth defect of the foot and ankle.
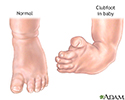
Clubfoot
Clubfoot is a condition that involves both the foot and lower leg in which the foot turns inward and downward. It is a congenital condition, which m...

Description
The type of surgery that is done depends on:
- How serious the clubfoot is
- Your child's age
- What other treatments your child has had
Your child will have general anesthesia (asleep and pain-free) during the surgery.
Ligaments are tissues that help hold the bones together in the body. Tendons are tissues that help attach muscles to bones. A clubfoot occurs when tight tendons and ligaments prevent the foot from stretching into the right position.
To repair a clubfoot, 1 or 2 cuts are made in the skin, most often on the back of the foot and around the inside part of the foot.
- Your child's surgeon may make the tendons around the foot longer or shorter. The Achilles tendon at the back of the foot is almost always cut or lengthened.
- Older children or more severe cases may need some bone cuts. Sometimes, pins, screws or plates are placed in the bones of the foot.
- A cast is placed on the foot after surgery to keep it in position while it heals. Sometimes a splint is put on first, and the cast is placed a few days later.
Older children who still have a foot deformity after surgery may need more surgery. Also, children who have not had surgery yet may need surgery as they grow. Types of surgery they may need include:
- Osteotomy: Removing part of the bone.
- Fusion or arthrodesis: Two or more bones are fused together. The surgeon may use bone from somewhere else in the body.
- Metal pins, screws or plates may be used to hold the bones together for a while.
Why the Procedure Is Performed
A baby who is born with a clubfoot is first treated with a cast to stretch the foot into a more normal position.
- A new cast will be placed every week so the foot can be stretched into position.
- Cast changes continue for about 2 months. After casting, the child wears a brace for several years.
Clubfoot found in babies can often be successfully managed with casting and bracing, thereby avoiding surgery.
However, clubfoot repair surgery may be needed if:
- The cast or other treatments do not fully correct the problem.
- The problem comes back.
- A clubfoot was never treated.
Risks
Risks from any anesthesia and surgery are:
- Breathing problems
- Reactions to medicines
- Bleeding
- Infection
Possible problems from clubfoot surgery are:
- Damage to nerves in the foot
- Foot swelling
- Problems with blood flow to the foot
- Wound healing problems
- Stiffness
-
Arthritis
Arthritis
Arthritis is inflammation or degeneration of one or more joints. A joint is the area where 2 bones meet. There are more than 100 different types of...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Weakness
Before the Procedure
Your child's surgeon will:
- Take a medical history of your child
- Do a complete physical exam of your child
- Order x-rays of the clubfoot
- Test your child's blood, if needed (for example, do a complete blood count and check electrolytes or clotting factors)
Complete blood count
A complete blood count (CBC) test measures the following:The number of white blood cells (WBC count)The number of red blood cells (RBC count)The numb...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Always tell your child's surgeon or nurse:
- Medicines your child is taking
- Herbs, and vitamins your child is taking without a prescription
During the week before your surgery:
- You may be asked to temporarily stop giving your child medicines that keep their blood from clotting. These medicines are called blood thinners. This includes over-the-counter medicines and supplements such as aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), and vitamin E. Many prescription medicines are also blood thinners.
- Ask your child's surgeon which medicines they should still take on the day of surgery.
On the day of the surgery:
- Follow instructions about when your child should stop eating and drinking.
- Give your child the medicines their surgeon told you to give them with a small sip of water.
- Arrive at the hospital on time.
After the Procedure
Depending on the surgery that is done, your child may go home on the same day or stay in the hospital for 1 to 3 days right after the surgery. The hospital stay may be longer if surgery was also done on the bones.
Your child's foot should be kept in a raised position. Medicines may be prescribed to help control the pain.
The skin around your child's cast will be checked often to make sure it stays pink and healthy. Your child's toes also will be checked to make sure they are pink and your child can move and feel them. These are signs of proper blood flow.
Your child will have a cast on for 6 to 12 weeks. It may be changed several times. Before your child leaves the hospital, you will be taught how to take care of the cast.
When the last cast is taken off, your child will probably be prescribed a brace, and may be referred for physical therapy. The therapist will teach you exercises to do with your child to strengthen the foot and make sure it stays flexible.
Outlook (Prognosis)
After recovering from surgery, your child's foot will be in a much better position. Your child should be able to have a normal, active life, including playing sports. But the foot may be stiffer than a foot that has not been treated with surgery.
In most cases of clubfoot, if only one side is affected, the child's foot and calf will be smaller than normal for the rest of the child's life.
Children who have had clubfoot surgery may need another surgery later in life.
References
Herring JA. Orthopaedic-related syndromes. In: Herring JA, ed. Tachdjian's Pediatric Orthopaedics. 6th ed. Philadelphia, PA: Elsevier; 2022:chap 37.
Kelly DM. Congenital anomalies of the lower extremity. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 29.
. Correction of clubfoot is required for normal ambulation later in life.</p>")



Review Date: 1/1/2025
Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.