
Congenital diaphragmatic hernia repair
Diaphragmatic hernia - surgeryCongenital diaphragmatic hernia (CDH) repair is surgery to close an opening or space in a baby's diaphragm. This opening is called a hernia. It is a rare type of birth defect. Congenital means the problem is present at birth.
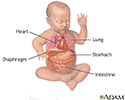
Congenital diaphragmatic hernia
A diaphragmatic hernia is a birth defect in which there is an abnormal opening in the diaphragm. The diaphragm is the muscle between the chest and a...

Description
Until the surgery is done, and usually for some time afterwards, nearly all infants need a breathing machine to improve their oxygen levels. Many babies with CDH will require extracorporeal membrane oxygenation (ECMO), which uses a pump to circulate blood through an artificial lung and back into the bloodstream of the baby.
Extracorporeal membrane oxygenation
Extracorporeal membrane oxygenation (ECMO) is a treatment that uses a pump to circulate blood through an artificial lung back into the bloodstream of...

The surgery is done while your child is under general anesthesia (asleep and not able to feel pain). The surgeon usually makes a cut (incision) in the belly under the lower ribs. This allows the organs in the area to be reached. The surgeon gently pulls these organs down into place through the opening in the diaphragm and into the abdominal cavity.
General anesthesia
General anesthesia is treatment with certain medicines that puts you into a deep sleep-like state so you do not feel pain during surgery. After you ...
Read Article Now Book Mark ArticleIn less severe cases, the surgery can be done using smaller incisions in the chest. A small video camera called a thoracoscope is placed through one of the incisions. This allows the surgeon to view inside the chest. Instruments to repair the hole in the diaphragm are placed through the other incisions.
In either type of operation, the surgeon repairs the hole in the diaphragm. If the hole is small, it may be repaired with stitches. Otherwise, an artificial patch is used to cover the hole.
Why the Procedure Is Performed
The diaphragm is a muscle. It is essential for normal breathing. It separates the chest cavity (where the heart and lungs are) from the belly area.
In a child with CDH, the diaphragm muscle is not completely formed and there is an abnormally large opening. The CDH opening allows organs from the belly (stomach, spleen, liver, and intestines) to go up into the chest cavity where the lungs are. This can prevent the lungs from growing and developing normally in the womb. The blood vessels in the lungs can also develop abnormally. This can cause difficulty breathing both before and after the repair surgery. It can result in not enough oxygen getting into the baby's body.
Depending on how much space in the chest is taken up by the abdominal organs, and when this happened during development in the womb, there can be varying outcomes.
A diaphragmatic hernia can be life threatening and most babies with CDH are very ill. Surgery to repair CDH must be done as early as possible after the baby is born. Even after surgery, some babies' lungs are not able to function on their own because they are so underdeveloped.
Risks
Risks for this surgery include:
- Breathing problems, which may be severe
Breathing problems
Breathing difficulty may involve:Difficult breathing Uncomfortable breathingFeeling like you are not getting enough air
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Bleeding
Bleeding
Bleeding is the loss of blood. Bleeding may be:Inside the body (internal)Outside the body (external)Bleeding may occur:Inside the body when blood le...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Collapsed lung
Collapsed lung
A collapsed lung occurs when air escapes from the lung. The air then fills the space outside of the lung between the lung and chest wall. This buil...
ImageRead Article Now Book Mark Article - Lung problems that do not go away
- Infection
- Reactions to medicines
Before the Procedure
Babies born with CDH usually need a breathing tube following birth and are admitted to a neonatal intensive care unit (NICU). It may be days or weeks before the baby is stable enough for surgery. Because the condition is life threatening and transporting a very ill newborn is risky, babies who are known to have CDH should be delivered in a center with pediatric surgeons and neonatologists.
- In the NICU, your baby will probably need a breathing machine (mechanical ventilator) before the surgery. This helps the baby breathe.
Mechanical ventilator
A mechanical ventilator is a machine that helps with breathing. This article discusses the use of mechanical ventilators in infants.
Read Article Now Book Mark Article - If your child is very sick, a heart-lung bypass machine (ECMO) may be needed to do the work of the heart and lungs.
- Before surgery, your baby will have x-rays and regular blood tests to see how well the lungs are working. A light sensor (called a pulse oximeter) is taped to your baby's skin to monitor the oxygen level in the blood.
x-rays
X-rays are a type of electromagnetic radiation, just like visible light. An x-ray machine sends individual x-ray waves through the body. The images...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Your baby may be given medicines to regulate blood pressure and stay comfortable.
Your baby will have tubes placed:
- From the mouth or nose to the stomach to keep air out of the stomach
- In an artery to monitor blood pressure
- In a vein to deliver nutrients and medicines
After the Procedure
Your baby will be on a breathing machine after the surgery and will stay in the hospital for several weeks. Once taken off the breathing machine, your baby may still need oxygen and medicines for a while.
Feedings will start after your baby's bowels start working. Feedings are usually given through a small, soft feeding tube from the mouth or nose into the stomach or small intestine until your baby can take milk by mouth.
Nearly all infants with CDH have reflux when they eat. This means the food or acid in their stomach moves up into their esophagus, the tube that leads from the throat to the stomach. This can be uncomfortable. It also leads to frequent spitting up and vomiting, which makes feedings more difficult once your baby is taking food by mouth. Reflux increases the risk for pneumonia if babies inhale milk into their lungs. It can also make it challenging for babies to take in enough calories to grow.
Reflux
Gastroesophageal reflux occurs when stomach contents leak backward from the stomach into the esophagus. This causes "spitting up" in infants....

The nurses and feeding specialists will teach you ways to hold and feed your baby to prevent reflux. Some babies need to be on a feeding tube for a long time to help them get enough calories to grow.
Outlook (Prognosis)
The outcome of this surgery depends on how well your baby's lungs have developed. Some babies have other medical problems, especially with their heart, brain, muscles, and joints, which often affect how well the baby does.
Usually the outlook is good for infants who have well-developed lung tissue and no other problems. Even so, most babies who are born with a diaphragmatic hernia are very ill and will stay in the hospital for a long time. With advances in medicine, the outlook for these infants is improving.
All babies who have had CDH repairs will need to be watched closely to make sure the hole in their diaphragm does not open up again as they grow.
Babies who had a large opening or defect in the diaphragm, or who had more problems with their lungs after birth, may have lung disease after they leave the hospital. They may need oxygen, medicines, and a feeding tube for months or years.
Some babies will have problems crawling, walking, talking, and eating. They will need to see physical or occupational therapists to help them develop muscles and strength.
References
Acharya KK, Sprecher AJ, Cohen SS. Diaphragmatic hernia. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 131.
Centers for Disease Control and Prevention website. Birth defects. Diaphragmatic hernia. www.cdc.gov/birth-defects/about/diaphragmatic-hernia.html. Updated November 19, 2024. Accessed May 19, 2025.
Harting MT, Hollinger LE, Lally KP. Congenital diaphragmatic hernia and eventration. In: Holcomb GW, Murphy JP, St. Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, PA: Elsevier; 2020:chap 24.
Lee SY, Jackson JE, Lakshiminrusimha S, Brown EG, Farmer DL. Anatomic disorders of the chest and airways. In: Gleason CA, Sawyer T, eds. Avery's Diseases of the Newborn. 11th ed. Philadelphia, PA: Elsevier; 2024:chap 44.

 shortly after birth; Prenatal ultrasound often identifies a diaphragmatic hernia.</p>")



Review Date: 10/17/2024
Reviewed By: Mary J. Terrell, MD, IBCLC, Neonatologist, Cape Fear Valley Medical Center, Fayetteville, NC. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. Editorial update 05/19/2025.
 All rights reserved.
All rights reserved.