
Tracheoesophageal fistula and esophageal atresia repair
TEF repair; Esophageal atresia repairTracheoesophageal fistula and esophageal atresia repair is surgery to repair two birth defects in the esophagus and trachea. The defects usually occur together.
Description
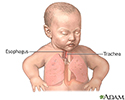
The esophagus is the tube that carries food from the mouth to the stomach. The trachea (windpipe) is the tube that carries air into and out of the lungs.
The defects usually occur together. They may occur along with other problems as part of a syndrome (group of problems):
- Esophageal atresia (EA) occurs when the upper part of the esophagus does not connect with the lower esophagus and stomach.
Esophageal atresia
Esophageal atresia is a birth defect in which the esophagus does not develop properly. The esophagus is the tube that normally carries food from the...
Read Article Now Book Mark Article - Tracheoesophageal fistula (TEF) is an abnormal connection between the upper part of the esophagus and the trachea or windpipe.
This surgery is almost always done soon after birth. Both defects can often be repaired at the same time. Briefly, the surgery takes place this way:
- Medicine (anesthesia) is given so that the baby is in a deep sleep and pain-free during surgery.
- The surgeon makes a cut on the side of the chest between the ribs.
- The fistula between the esophagus and windpipe is closed.
- The upper and lower portions of the esophagus are sewn together if possible.
Often the two parts of the esophagus are too far apart to sew together right away. In this case:
- Only the fistula is repaired during the first surgery.
- A gastrostomy tube (a tube that goes through the skin into the stomach) may be placed to give your child nutrition.
- Your child will have another surgery later to repair the esophagus.
Sometimes the surgeon will wait 2 to 4 months before doing the surgery. Waiting allows your baby to grow or have other problems treated. If your child's surgery is delayed:
- A gastrostomy tube (G-tube) will be placed through the abdominal wall into the stomach. Numbing medicines (local anesthesia) will be used so that the baby does not feel pain.
Gastrostomy tube
A gastrostomy feeding tube insertion is the placement of a feeding tube through the skin and the stomach wall. It goes directly into the stomach....
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - At the same time the tube is placed, the doctor may widen the baby's esophagus with a special instrument called a dilator. This will make the future surgery easier. This process may need to be repeated, sometimes several times, before repair is possible.
Why the Procedure Is Performed
Tracheoesophageal fistula and esophageal atresia are life-threatening problems. They need to be treated right away. If these problems are not treated:
- Your child may breathe saliva and fluids from the stomach into the lungs. This is called aspiration. It can cause choking and pneumonia (lung infection).
- Your child cannot swallow and digest at all if the esophagus does not connect to the stomach.
Risks
Risks of anesthesia and surgery in general include:
- Reactions to medicines
- Breathing problems
Breathing problems
Breathing difficulty may involve:Difficult breathing Uncomfortable breathingFeeling like you are not getting enough air
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Bleeding, blood clots, or infection
Bleeding
Bleeding is the loss of blood. Bleeding may be:Inside the body (internal)Outside the body (external)Bleeding may occur:Inside the body when blood le...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Risks of this surgery include:
- Collapsed lung (pneumothorax)
Pneumothorax
A collapsed lung occurs when air escapes from the lung. The air then fills the space outside of the lung between the lung and chest wall. This buil...
ImageRead Article Now Book Mark Article - Food leakage from the area that is repaired
- Low body temperature (hypothermia)
Hypothermia
Hypothermia is dangerously low body temperature, below 95°F (35°C).
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Narrowing of the repaired organs
- Reopening of the fistula
Before the Procedure
Your baby will be admitted to the neonatal intensive care unit (NICU) as soon as the doctors diagnose either of these problems.
Your baby will receive nutrition by vein (intravenous, or IV) and may also be on a breathing machine (ventilator). The care team may use suction to keep fluids from going into the lungs.
Some infants who are premature, have a low birth weight, or have other birth defects beside TEF and/or EA may not be able to have surgery until they grow larger or until other problems have been treated or have gone away.
After the Procedure
After surgery, your child will be cared for in the hospital's NICU.
Additional treatments after surgery usually include:
- Antibiotics as needed, to prevent infection
- Breathing machine (ventilator)
- Chest tube (a tube through the skin into the chest wall) to drain fluids from the space between the outside of the lung and the inside of the chest cavity
- Intravenous (IV) fluids, including nutrition
Intravenous
Intravenous means "within a vein. " Most often it refers to giving medicines or fluids through a needle or tube inserted into a vein. This allows th...
Read Article Now Book Mark Article - Oxygen
- Pain medicines as needed
If both the TEF and EA are repaired:
- A tube is placed through the nose into the stomach (nasogastric tube) during the surgery.
- Feedings are usually started through this tube a few days after surgery.
- Feedings by mouth are started slowly. The baby may need feeding therapy.
If only the TEF is repaired, a G-tube is used for feedings until the atresia can be repaired. The baby may also need continuous or frequent suction to clear secretions from the upper esophagus.
While your baby is in the hospital, the care team will show you how to use and replace the G-tube. You may also be sent home with an extra G-tube. The hospital staff will inform a home health supply company of your equipment needs.
How long your infant stays in the hospital depends on the type of defect your child has and whether there are other problems in addition to the TEF and EA. You will be able to bring your baby home once they are taking feedings by mouth or gastrostomy tube, is gaining weight, and safely breathing on their own.
Outlook (Prognosis)
Surgery can usually repair a TEF and EA. Once healing from the surgery is complete, your child may have these problems:
- The part of the esophagus that was repaired may become narrower. Your child may need to have more surgery to treat this.
- Your child may have heartburn, or gastroesophageal reflux (GERD). This occurs when acid from the stomach goes up into the esophagus. GERD may cause breathing problems.
During infancy and early childhood, many children will have problems with breathing, growth, and feeding, and will need to continue seeing both their primary care provider and specialists.
Babies with TEF and EA who also have defects of other organs, most commonly the heart, may have long-term health problems.
References
Madanick R, Kaila V. Anatomy, histology, embryology, and developmental anomalies of the esophagus. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 43.
Rothenberg SS. Esophageal atresia and tracheoesophageal fistula malformations. In: Holcomb GW, Murphy P, St. Peter SD, eds. Holcomb and Ashcraft's Pediatric Surgery. 7th ed. Philadelphia, PA: Elsevier; 2020:chap 27.



, in order to decompress the stomach and prevent fluid in the stomach from flowing up the esophagus, through the fistula and into the lungs. The infant is then cared for in an intensive care unit until he or she is well enough to undergo resection of the fistula and a definitive repair of the esophagus.</p>")
 to keep warm. They may require oxygen and/or mechanical ventilation. A chest tube may be in place to drain fluids. Intravenous fluids and pain medications will be given. Feedings will be started as soon as possible, depending on the extent of the repair. Length of the hospitalization varies, depending on the seriousness of the surgery and the baby's condition.</p>")
Review Date: 11/9/2021
Reviewed By: Kimberly G. Lee, MD, MSc, IBCLC, Clinical Professor of Pediatrics, Division of Neonatology, Medical University of South Carolina, Charleston, SC. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.