
Miscarriage
Abortion - spontaneous; Spontaneous abortion; Abortion - missed; Abortion - incomplete; Abortion - complete; Abortion - inevitable; Abortion - infected; Missed abortion; Incomplete abortion; Complete abortion; Inevitable abortion; Infected abortionA miscarriage is the spontaneous loss of a fetus before the 20th week of pregnancy. Pregnancy losses after the 20th week are called stillbirths. Miscarriage is a naturally occurring event, unlike medicine abortions or abortion procedures.
Stillbirths
A stillbirth is when a baby dies in the womb during the last 20 weeks of pregnancy. A miscarriage is a fetal loss in the first half of pregnancy...
Read Article Now Book Mark ArticleMedicine abortions
A medication abortion is the use of medicine to end an undesired pregnancy. The medicine helps remove the fetus and placenta to leave the woman's wo...
Read Article Now Book Mark ArticleAbortion procedures
An abortion is a medical procedure that ends an undesired pregnancy by removing the fetus and placenta from the woman's uterus (womb). A medication ...

A miscarriage may also be called a "spontaneous abortion." Other terms for the early loss of pregnancy include:
- Complete abortion: All of the products (tissue) of conception leave the body.
- Incomplete abortion: Only some of the products of conception leave the body.
- Inevitable abortion: Symptoms cannot be stopped and a miscarriage will happen.
- Infected (septic) abortion: The lining of the uterus and any remaining products of conception become infected.
- Missed abortion: The pregnancy has failed and the products of conception do not leave the body.
Your health care provider may also use the term "threatened miscarriage." The symptoms of this condition are abdominal cramps with or without vaginal bleeding. They are a sign that a miscarriage may occur.
Threatened miscarriage
A threatened miscarriage is a condition that indicates the potential for a miscarriage or early pregnancy loss. It might take place before the 20th ...

Abdominal cramps
Abdominal pain is pain that you feel anywhere between your chest and groin. This is often referred to as the stomach region or belly.

Causes
Most miscarriages are caused by chromosome problems that make it impossible for the fetus to develop. In rare cases, these problems are related to the mother's or father's genes.
Other possible causes of miscarriage may include:
- Drug or alcohol use
Alcohol use
Pregnant women are strongly urged not to drink alcohol during pregnancy. Drinking alcohol while pregnant has been shown to cause harm to a baby as it...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Blood clotting disorders
- Exposure to environmental toxins
- Hormone problems
- Infection
- Obesity
Obesity
Obesity means weighing more than what is healthy for a given height. Obesity is a serious, chronic disease. It can lead to other health problems, i...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Physical problems with the mother's reproductive organs
- Problem with the body's immune response
- Serious body-wide (systemic) diseases in the mother (such as uncontrolled diabetes)
Systemic
Systemic means affecting the entire body, rather than a single organ or body part. For example, systemic disorders, such as high blood pressure, or s...
Read Article Now Book Mark ArticleDiabetes
Diabetes is a long-term (chronic) disease in which the body cannot regulate the amount of sugar in the blood.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Smoking
Around half of all fertilized eggs die and are lost (aborted) spontaneously, usually before the woman knows she is pregnant. Among women who know they are pregnant, about 10% to 25% will have a miscarriage. Most miscarriages occur during the first 7 weeks of pregnancy. The rate of miscarriage drops after the fetus's heartbeat is detected.
The risk for miscarriage is higher:
- In women who are older -- The risk increases after 30 years of age and becomes even greater between 35 and 40 years, and is highest after age 40.
- In women who have already had one or more miscarriages.
Symptoms
Possible symptoms of miscarriage may include:
- Low back pain or abdominal pain that is dull, sharp, or cramping
- Tissue or clot-like material that passes from the vagina
- Vaginal bleeding, with or without abdominal cramps
Some women may not have any symptoms at the beginning.
Exams and Tests
During a pelvic exam, your provider may see that your cervix has opened (dilated).
Cervix
The cervix is the lower end of the womb (uterus). It is at the top of the vagina. It is about 2. 5 to 3. 5 centimeters (1 to 1. 3 inches) long. Th...

Abdominal or vaginal ultrasound may be done to check the fetus's development and heartbeat, and the amount of your bleeding.
Abdominal
Abdominal ultrasound is a type of imaging test. It is used to look at organs in the abdomen, including the liver, gallbladder, pancreas, and kidneys...

Vaginal ultrasound
Transvaginal ultrasound is a test used to look at a woman's uterus, ovaries, tubes, cervix, and pelvic area. Transvaginal means across or through the...

The following blood tests may be performed:
- Blood type (if you have an Rh-negative blood type, you would require a treatment with Rho(D)-immune globulin [RhoGAM and other brands]).
Rho(D)-immune globulin [RhoGAM and othe...
Rh incompatibility is a condition that develops when a pregnant woman has Rh-negative blood and the baby in her womb has Rh-positive blood.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Complete blood count (CBC) to determine how much blood has been lost.
Complete blood count
A complete blood count (CBC) test measures the following:The number of white blood cells (WBC count)The number of red blood cells (RBC count)The numb...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - HCG (qualitative) to confirm pregnancy.
HCG (qualitative)
A qualitative human chorionic gonadotropin (HCG or hCG) blood test checks if there is a hormone called human chorionic gonadotropin in your blood. H...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - HCG (quantitative) done every several days or weeks.
HCG (quantitative)
A quantitative human chorionic gonadotropin (HCG or hCG) blood test measures the specific level of HCG in the blood. HCG is a hormone produced in th...
ImageRead Article Now Book Mark Article - White blood count (WBC) and differential to check for infection.
WBC
A WBC count is a blood test to measure the number of white blood cells (WBCs) in the blood. It is a part of a complete blood count (CBC). WBCs are a...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleDifferential
The blood differential test measures the percentage of each type of white blood cell (WBC) that you have in your blood. It also reveals if there are...
ImageRead Article Now Book Mark Article
Treatment
When a miscarriage occurs, the tissue passed from the vagina should be examined. This is done to determine if it was a normal placenta or a rare condition known as a hydatidiform mole. It is also important to find out whether any pregnancy tissue remains in the uterus. In rare cases an ectopic pregnancy can look like a miscarriage. If you have passed tissue, ask your provider if the tissue should be sent for genetic testing. This can be helpful to determine if a treatable cause of miscarriage is present.
Hydatidiform mole
Hydatidiform mole (HM) is a rare mass or growth that forms inside the womb (uterus) at the beginning of a pregnancy. It is a type of gestational tro...

If the pregnancy tissue does not naturally leave the body, you may be closely watched for up to 2 weeks. You may need a procedure (suction curettage, D and C) or medicine to remove the remaining contents from your uterus.
Suction curettage, D and C
An abortion is a medical procedure that ends an undesired pregnancy by removing the fetus and placenta from the woman's uterus (womb). A medication ...
After treatment, women usually resume their normal menstrual cycle within 4 to 6 weeks. Any further vaginal bleeding should be carefully monitored. It is often possible to become pregnant immediately. It is suggested that you wait one normal menstrual cycle before trying to become pregnant again.
Possible Complications
In rare cases, complications of miscarriage can occur.
An infected abortion may occur if any tissue from the placenta or fetus remains in the uterus after the miscarriage. Symptoms of an infection include fever, vaginal bleeding that does not stop, cramping, and a foul-smelling vaginal discharge. Infections can be serious and need immediate medical attention.
Women who lose a fetus after 20 weeks of pregnancy receive different medical care. This is called premature delivery or fetal demise. This needs immediate medical attention.
Premature delivery
A premature infant is a baby born before 37 full weeks of gestation (more than 3 weeks before the due date).
Read Article Now Book Mark ArticleAfter a miscarriage, women and their partners may feel sad. This is normal. If your feelings of sadness do not go away or get worse, seek advice from family and friends as well as your provider. However, for most couples, a history of a miscarriage doesn't reduce the chances of having a healthy baby in the future.
When to Contact a Medical Professional
Contact your provider if you:
- Have vaginal bleeding with or without cramping during pregnancy.
- Are pregnant and notice tissue or clot-like material that passes through your vagina. Collect the material and bring it to your provider for examination.
Prevention
Early, complete prenatal care is the best prevention for complications of pregnancy, such as miscarriage.
Miscarriages that are caused by systemic diseases can be prevented by detecting and treating the disease before pregnancy occurs.
Miscarriages are also less likely if you avoid things that are harmful to your pregnancy. These include x-rays, recreational drugs, alcohol, high caffeine intake, and infectious diseases.
When a mother's body has difficulty keeping a pregnancy, signs such as slight vaginal bleeding may occur. This means there is a risk for miscarriage. But it does not mean one will definitely occur. A pregnant woman who develops any signs or symptoms of threatened miscarriage should contact her prenatal provider instantly.
Threatened miscarriage
A threatened miscarriage is a condition that indicates the potential for a miscarriage or early pregnancy loss. It might take place before the 20th ...
Taking a prenatal vitamin which contains folic acid before you become pregnant and during pregnancy can greatly lower the chances of miscarriage and certain birth defects.
References
American College of Obstetricians and Gynecologists website. ACOG Guide to Language and Abortion. www.acog.org/contact/media-center/abortion-language-guide. Updated October 2024. Accessed November 28, 2024.
Henn MC, Lall MD. Complications of pregnancy. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 173.
Jauniaux ERM, Simpson JL. Pregnancy loss. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 8th ed. Philadelphia, PA: Elsevier; 2021:chap 33.
Reddy UM, Silver RM. Stillbirth. In: Lockwood CJ, Copel JA, Dugoff L, et al, eds. Creasy and Resnik's Maternal-Fetal Medicine: Principles and Practice. 9th ed. Philadelphia, PA: Elsevier; 2023:chap 42.
Turocy J, Williams Z. Early and recurrent pregnancy loss; etiology, diagnosis, treatment. In: Gershenson DM, Lentz GM, Valea FA, Lobo RA, eds. Comprehensive Gynecology. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 16.
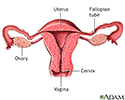
Normal uterine anatomy (cut section) - illustration
The uterus is a muscular organ with thick walls, two upper openings to the fallopian tubes and an inferior opening to the vagina.
Normal uterine anatomy (cut section)
illustration
Review Date: 10/15/2024
Reviewed By: John D. Jacobson, MD, Professor Emeritus, Department of Obstetrics and Gynecology, Loma Linda University School of Medicine, Loma Linda, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.