
Hiatal hernia
Hernia - hiatalHiatal hernia is a condition in which part of the stomach extends through an opening of the diaphragm into the chest. The diaphragm is the sheet of muscle that divides the chest from the abdomen.
Causes
The exact cause of hiatal hernia is not known. The condition may be due to weakness of the supporting tissue. Your risk for the problem goes up with age, obesity, and smoking. Hiatal hernias are very common. The problem occurs often in people over 50 years of age.
Obesity
Overweight and obesity mean having a weight than is higher than what is healthy for a given height. A person may be overweight from extra muscle, bo...

This condition may be linked to reflux (backflow) of gastric acid from the stomach into the esophagus.
Reflux
Gastroesophageal reflux disease (GERD) is a condition in which the stomach contents leak backward from the stomach into the esophagus (food pipe). F...

Children with this condition are most often born with it (congenital). In infants, it often occurs with gastroesophageal reflux.
Gastroesophageal reflux
Anti-reflux surgery is surgery to tighten the muscles at the bottom of the esophagus (the tube that carries food from the mouth to the stomach). Pro...
Read Article Now Book Mark ArticleSymptoms
Symptoms may include:
-
Chest pain
Chest pain
Chest pain is discomfort or pain that you feel anywhere along the front of your body between your neck and upper abdomen.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Heartburn, worse when bending over or lying down
Heartburn
Heartburn is a painful burning feeling just below or behind the breastbone. Most of the time, it comes from the esophagus. The pain often rises in ...
ImageRead Article Now Book Mark Article - Swallowing difficulty
A hiatal hernia by itself rarely causes symptoms. Pain and discomfort are due to the upward flow of stomach acid, air, or bile.
Exams and Tests
Tests that may be used include:
-
Barium swallow x-ray
Barium swallow x-ray
An upper GI and small bowel series is a set of x-rays taken to examine the esophagus, stomach, and small intestine. Barium enema is a different test ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Esophagogastroduodenoscopy (EGD)
EGD
Esophagogastroduodenoscopy (EGD) is a test to examine the lining of the esophagus, stomach, and first part of the small intestine (the duodenum)....
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Treatment
The goals of treatment are to relieve symptoms and prevent complications. Treatments may include:
- Medicines to control stomach acid
-
Surgery to repair the hiatal hernia and prevent reflux
Surgery to repair the hiatal hernia
Anti-reflux surgery is a treatment for acid reflux, also known as GERD (gastroesophageal reflux disease). GERD is a condition in which food or stoma...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Other measures to reduce symptoms include:
- Avoiding large or heavy meals
- Not lying down or bending over right after a meal
- Reducing weight and not smoking
- Raising the head of the bed 4 to 6 inches (10 to 15 centimeters)
If medicines and lifestyle measures do not help control symptoms, you may need surgery.
Outlook (Prognosis)
Treatment can relieve most symptoms of hiatal hernia.
Possible Complications
Complications may include:
- Pulmonary (lung) aspiration
Aspiration
Aspiration means to draw in or out using a sucking motion. It has two meanings:Breathing in a foreign object (for example, sucking food into the air...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Slow bleeding and iron deficiency anemia (due to a large hernia)
Iron deficiency anemia
Anemia is a condition in which the body does not have enough healthy red blood cells. Red blood cells provide oxygen to body tissues. There are man...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Strangulation (closing off) of the hernia (very uncommon)
When to Contact a Medical Professional
Contact your health care provider if:
- You have symptoms of a hiatal hernia.
- You have a hiatal hernia and your symptoms get worse or do not improve with treatment.
- You develop new symptoms.
Prevention
Controlling risk factors such as obesity may help prevent hiatal hernia.
References
Battafarano RJ. Esophagus: Management of paraesophageal hernia repair. In: Cameron J, ed. Current Surgical Therapy. 14th ed. Philadelphia, PA: Elsevier; 2023:3-80.
Falk GW, Katzka DA. Diseases of the esophagus. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier; 2020:chap 129.
Lord KA, Lippincott J. Hiatal hernia. In: Ferri FF, ed. Ferri's Clinical Advisor 2023. Philadelphia, PA: Elsevier; 2023:749.e2-749.e5.
Yates RB, Oelschlager BK. Gastroesophageal reflux disease and hiatal hernia. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. St Louis, MO: Elsevier; 2022:chap 43.
-
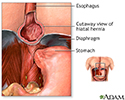
Hiatal hernia - X-ray - illustration
This X-ray shows the upper portion of the stomach protruding through the diaphragm (hiatal hernia).
Hiatal hernia - X-ray
illustration
-
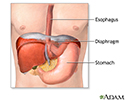
Hiatal hernia - illustration
A hiatal hernia occurs when part of the stomach protrudes up into the chest through the sheet of muscle called the diaphragm. This may result from a weakening of the surrounding tissues and may be aggravated by obesity and/or smoking.
Hiatal hernia
illustration
-
Hiatal hernia repair - series
Presentation


 in the muscle between the abdomen and chest (diaphragm) is too large, some of the stomach can slip up into the chest cavity. This can cause heartburn (gastro-esophageal reflux; GER) as gastric acid backflows from the stomach into the esophagus. Hiatal hernia repair is surgery to repair a bulging of stomach tissue through the muscle between the abdomen and chest (diaphragm) into the chest (hiatal hernia). Hiatal hernia repair may be recommended when the patient has severe heartburn, severe inflammation of the esophagus from the backflow of gastric fluid (reflux), narrowing of the opening (hiatus) through the diaphragm (esophageal stricture), chronic inflammation of the lungs (pneumonia) from frequent breathing in (aspiration) of gastric fluids.</p>")
, an incision is made in the abdomen. </p>")
 is tightened and the stomach is stitched in position to prevent reflux. The upper part of the stomach (fundus) may be wrapped around the esophagus (fundoplication) to reduce reflux.</p>")
 during surgery and may remain for a few days. Small, frequent feedings are recommended. </p>")
-
Hiatal hernia - X-ray - illustration
This X-ray shows the upper portion of the stomach protruding through the diaphragm (hiatal hernia).
Hiatal hernia - X-ray
illustration
-
Hiatal hernia - illustration
A hiatal hernia occurs when part of the stomach protrudes up into the chest through the sheet of muscle called the diaphragm. This may result from a weakening of the surrounding tissues and may be aggravated by obesity and/or smoking.
Hiatal hernia
illustration
-
Hiatal hernia repair - series
Presentation
Review Date: 5/2/2023
Reviewed By: Michael M. Phillips, MD, Emeritus Professor of Medicine, The George Washington University School of Medicine, Washington, DC. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.