
Febrile seizures
Seizure - fever induced; Febrile convulsionsA febrile seizure is a convulsion in a child triggered by a fever.
Convulsion
A seizure is the physical changes in behavior that occurs during an episode of specific types of abnormal electrical activity in the brain. The term ...

Fever
Fever is the temporary increase in the body's temperature in response to a disease or illness. A child has a fever when the temperature is at or abov...

Causes
A temperature of 100.4°F (38°C) or above may cause febrile seizures in children.
A febrile seizure can be frightening for any parent or caregiver. Most of the time, a febrile seizure does not cause any harm. The child usually does not have a more serious long-term health problem.
Febrile seizures occur most often in otherwise healthy children between ages 6 months and 5 years. Toddlers are most commonly affected. Febrile seizures often run in families.
Most febrile seizures occur in the first 24 hours of an illness. It may not occur when the fever is highest. A cold or viral illness may trigger a febrile seizure.
Symptoms
A febrile seizure may be as mild as the child's eyes rolling or limbs stiffening. A simple febrile seizure stops by itself within a few seconds to 10 minutes. It is often followed by a brief period of drowsiness or confusion.
Symptoms may include any of the following:
- Sudden tightening (contraction) of muscles on both sides of a child's body. The muscle tightening may last for several seconds or longer.
- The child may cry or moan.
- If standing, the child will fall.
- The child may vomit or bite their tongue.
- Sometimes, children do not breathe and may begin to turn blue.
- The child's body may then begin to jerk rhythmically. The child will not respond to the parent's voice.
- Urine may be passed.
A seizure lasting longer than 15 minutes, is in just one part of the body, or that occurs again during the same illness is not a normal febrile seizure.
The health care provider may diagnose febrile seizure if the child has a tonic-clonic seizure but does not have a history of seizure disorders (epilepsy). A tonic-clonic seizure involves the entire body. In infants and young children, it is important to rule out other causes of a first-time seizure, especially meningitis (bacterial infection of the covering of the brain and spinal cord).
Tonic-clonic seizure
Bilateral tonic-clonic seizure is a type of seizure that involves the entire body. It is also called grand mal seizure. The terms generalized seizu...

Meningitis
Meningitis is an infection of the membranes covering the brain and spinal cord. This covering is called the meninges.

Exams and Tests
With a typical febrile seizure, the examination usually is normal, other than symptoms of the illness causing the fever. Often, the child will not need a full seizure workup, which includes an EEG, head CT, and lumbar puncture (spinal tap).
EEG
An electroencephalogram (EEG) is a test to measure the electrical activity of the brain.
CT
A computed tomography (CT) scan is an imaging method that uses x-rays to create pictures of cross-sections of the body. Related tests include:Abdomin...

Lumbar puncture (spinal tap)
Cerebrospinal fluid (CSF) collection is a test to look at the fluid that surrounds the brain and spinal cord. CSF acts as a cushion, protecting the b...

Further testing may be needed if the child:
- Is younger than 9 months or older than 5 years
- Has a brain, nerve, or developmental disorder
- Had the seizure in only one part of the body
- Had the seizure last longer than 15 minutes
- Had more than one febrile seizure in 24 hours
- Has an abnormal finding when examined
Treatment
The aim of treatment is to manage the underlying cause. The following measures help keep the child safe during a seizure:
- Do not hold down the child or try to stop the seizure movements.
- Do not leave the child alone.
- Lay the child on the ground in a safe area. Clear the area of furniture or other sharp objects.
- Slide a blanket under the child if the floor is hard.
- Move the child only if they are in a dangerous location.
- Loosen tight clothing, especially around the neck. If possible, open or remove clothes from the waist up.
- If the child vomits or if saliva and mucus build up in the mouth, turn the child to the side or on the stomach. This is also important if it looks like the tongue is getting in the way of breathing.
- Do not force anything into the child's mouth to prevent biting the tongue. This increases the risk for injury.
If the seizure lasts several minutes, call 911 or the local emergency number to have an ambulance take your child to the hospital.
Contact your child's provider as soon as possible to describe your child's seizure.
After the seizure, the most important step is to identify the cause of the fever. The focus is on bringing the fever down. The provider may tell you to give your child medicines to reduce the fever. Follow instructions exactly on how much and how often to give your child the medicine. These medicines, however, do not reduce the chance of having febrile seizures in the future.
It is normal for children to sleep or be drowsy or confused for a short time right after a seizure.
Outlook (Prognosis)
The first febrile seizure can be frightening for parents. Most parents are afraid that their child will die or have brain damage. However, simple febrile seizures are harmless. There is no evidence that they cause death, brain damage, epilepsy, or learning problems.
Most children outgrow febrile seizures by age 5.
Few children have more than 3 febrile seizures in their lifetime. The number of febrile seizures is not related to future risk for epilepsy.
Children who would develop epilepsy anyway will sometimes have their first seizures during fevers. These seizures most often do not appear like a typical febrile seizure.
When to Contact a Medical Professional
If the seizure lasts several minutes, call 911 or the local emergency number to have an ambulance bring your child to the hospital.
If the seizure ends quickly, drive the child to an emergency room when it is over.
Take your child to their provider if:
- Repeated seizures occur during the same illness.
- This looks like a new type of seizure for your child.
Contact their provider if other symptoms occur before or after the seizure, such as:
- Abnormal movements, tremors, or problems with coordination
-
Agitation or confusion
Agitation
Agitation is an unpleasant state of extreme arousal. An agitated person may feel stirred up, excited, tense, confused, or irritable.
Read Article Now Book Mark ArticleConfusion
Confusion is the inability to think as clearly or quickly as you normally do. You may feel disoriented and have difficulty paying attention, remembe...
ImageRead Article Now Book Mark Article -
Drowsiness
Drowsiness
Drowsiness refers to feeling more sleepy than normal during the day. People who are drowsy may fall asleep when they do not want to or at times whic...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Nausea
Nausea
Nausea is feeling an urge to vomit. It is often called "being sick to your stomach. "Vomiting or throwing-up forces the contents of the stomach up t...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Rash
Rash
Rashes involve changes in the color, feeling or texture of your skin.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Prevention
Because febrile seizures can be the first sign of illness, it is often not possible to prevent them. A febrile seizure does not mean that your child is not getting the proper care.
Occasionally, a provider will prescribe a medicine called diazepam to prevent or treat febrile seizures that occur more than once. However, no drug is completely effective in preventing febrile seizures.
References
Abou-Khalil BW, Gallagher MJ, Macdonald RL. Epilepsies. In: Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 100.
Mick NW. Pediatric fever. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 161.
Mikati MA, Tchapyjnikov D. Seizures in childhood. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 611.
National Institute of Neurological Disorders and Stroke website. Febrile seizures. www.ninds.nih.gov/health-information/disorders/febrile-seizures. Updated July 19, 2024. Accessed September 8, 2024.
Seinfeld S, Shinnar S. Febrile seizures. In: Swaiman KF, Ashwal S, Ferriero DM, et al, eds. Swaiman's Pediatric Neurology: Principles and Practice. 6th ed. Philadelphia, PA: Elsevier; 2017:chap 65.
-
Grand mal seizure - illustration
A febrile seizure is a generalized tonic-clonic (grand mal) seizure that occurs in some children as a response to a fever. Febrile seizures are usually associated with rapidly rising fevers, and usually occur early in the fever rather than later.
Grand mal seizure
illustration
-
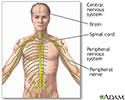
Central nervous system and peripheral nervous system - illustration
The central nervous system comprises the brain and spinal cord. The peripheral nervous system includes nerves outside the brain and spinal cord.
Central nervous system and peripheral nervous system
illustration

-
Grand mal seizure - illustration
A febrile seizure is a generalized tonic-clonic (grand mal) seizure that occurs in some children as a response to a fever. Febrile seizures are usually associated with rapidly rising fevers, and usually occur early in the fever rather than later.
Grand mal seizure
illustration
-
Central nervous system and peripheral nervous system - illustration
The central nervous system comprises the brain and spinal cord. The peripheral nervous system includes nerves outside the brain and spinal cord.
Central nervous system and peripheral nervous system
illustration
Review Date: 2/17/2024
Reviewed By: Charles I. Schwartz, MD, FAAP, Clinical Assistant Professor of Pediatrics, Perelman School of Medicine at the University of Pennsylvania, General Pediatrician at PennCare for Kids, Phoenixville, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team. Editorial update 09/08/2024.
 All rights reserved.
All rights reserved.