
Placenta previa
Vaginal bleeding - placenta previa; Pregnancy - placenta previaPlacenta previa is a problem of pregnancy in which the placenta grows in the lowest part of the womb (uterus) and covers all or part of the opening to the cervix.
Cervix
The cervix is the lower end of the womb (uterus). It is at the top of the vagina. It is about 2. 5 to 3. 5 centimeters (1 to 1. 3 inches) long. Th...

The placenta grows during pregnancy and feeds the developing baby. The cervix is the opening to the birth canal.
Causes
During pregnancy, the placenta moves as the womb stretches and grows. It is very common for the placenta to be low in the womb in early pregnancy. But as the pregnancy continues, the placenta moves to the top of the womb. By the third trimester, the placenta should be near the top of the womb, so the cervix is open for delivery.
Sometimes, the placenta partly or completely covers the cervix. This is called a placenta previa.
There are different forms of placenta previa:
- Marginal: The placenta is next to the cervix but does not cover the opening.
- Partial: The placenta covers part of the cervical opening.
- Complete: The placenta covers all of the cervical opening.
Placenta previa occurs in 1 out of 200 pregnancies. It is more common in women who have:
- An abnormally shaped uterus
- Had many pregnancies in the past
- Had multiple pregnancies, such as twins or triplets
- Scarring on the lining of the uterus due to a history of surgery, C-section, or abortion
- In vitro fertilization
- A history of placenta previa in a previous pregnancy
Women who smoke, use cocaine, or have their children at an older age may also have an increased risk.
Symptoms
The main symptom of placenta previa is sudden bleeding from the vagina. Some women also have cramps. The bleeding often starts near the end of the second trimester or beginning of the third trimester.
Sudden bleeding from the vagina
Vaginal bleeding in pregnancy is any discharge of blood from the vagina during pregnancy.

Bleeding may be severe and life threatening. It may stop on its own but can start again days or weeks later.
Labor sometimes starts within several days of the heavy bleeding. Sometimes, bleeding may not occur until after labor starts.
Exams and Tests
Your health care provider can diagnose this condition with a pregnancy ultrasound.
Treatment
Your provider will carefully consider the risk of bleeding against early delivery of your baby. After 36 weeks, delivery of the baby may be the best treatment.
Nearly all women with placenta previa will need a C-section. If the placenta covers all or part of the cervix, a vaginal delivery can cause severe bleeding. This can be deadly to both the mother and baby.
C-section
A C-section is the delivery of a baby by making an opening in the mother's lower belly area. It is also called a cesarean delivery.

If the placenta is near or covering part of the cervix, your provider may recommend:
- Reducing your activities
- Bed rest
- Pelvic rest, which means no sex, no tampons, and no douching
Nothing should be placed in your vagina.
You may need to stay in the hospital so your health care team can closely monitor you and your baby.
Other treatments you may receive:
- Blood transfusions
- Medicines to prevent early labor
- Medicines to help pregnancy continue to at least 36 weeks
- Shot of special medicine called Rhogam if your blood type is Rh-negative
- Steroid shots to help the baby's lungs mature
An emergency C-section may be done if the bleeding is heavy and cannot be controlled.
Outlook (Prognosis)
The biggest risk is severe bleeding that can be life threatening to the mother and baby. If you have severe bleeding, your baby may need to be delivered early, before major organs, such as the lungs, have developed.
For most women who receive regular prenatal care, this condition is diagnosed before symptoms appear. This helps the provider and mother take steps to minimize risks from this condition.
When to Contact a Medical Professional
Contact your provider if you have vaginal bleeding during pregnancy. Placenta previa can be dangerous to both you and your baby.
References
Francois KE, Foley MR. Antepartum and postpartum hemorrhage. In: Landon MB, Galan HL, Jauniaux ERM, et al, eds. Gabbe's Obstetrics: Normal and Problem Pregnancies. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 18.
Hull AD, Resnik R, Silver RM. Placenta previa and accreta, vasa previa, subchorionic hemorrhage, and abruptio placentae. In: Lockwood CJ, Copel JA, Dugoff L, et al, eds. Creasy and Resnik's Maternal-Fetal Medicine: Principles and Practice. 9th ed. Philadelphia, PA: Elsevier; 2023:chap 43.
Henn MC, Lall MD. Complications of pregnancy. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 173.
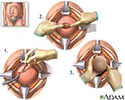
Cesarean section - illustration
1. The uterus is exposed through the abdominal wall, and an incision is made in the uterine covering. 2. The muscles of the uterus are separated, producing a hole for the delivery of the infant. 3. The infant is delivered through the opening in the uterine wall, after which, the uterus is stitched closed.
Cesarean section
illustration
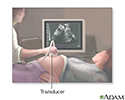
Ultrasound in pregnancy - illustration
The ultrasound has become a standard procedure used during pregnancy. It can demonstrate fetal growth and can detect increasing numbers of conditions including meningomyelocele, congenital heart disease, kidney abnormalities, hydrocephalus, anencephaly, club feet, and other deformities. Ultrasound does not produce ionizing radiation and is considered a very safe procedure for both the mother and the fetus.
Ultrasound in pregnancy
illustration
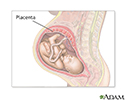
Anatomy of a normal placenta - illustration
The placenta provides the fetus with oxygen and nutrients and takes away waste such as carbon dioxide via the umbilical cord.
Anatomy of a normal placenta
illustration
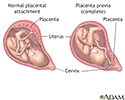
Placenta previa - illustration
Placenta previa is a condition of pregnancy when the placenta implants in the lower part of the uterus, partly or completely obstructing the cervical outlet to the vagina (birth canal).
Placenta previa
illustration
Placenta - illustration
In the placenta, nutrients, wastes, and gases are exchanged between the mothers blood and the babys blood.
Placenta
illustration
Ultrasound, normal fetus - arms and legs - illustration
This is a normal fetal ultrasound performed at 19 weeks gestation. This is the type of spilt-screen display you might see during an ultrasound, or if the technician prints a copy of the ultrasound for you. This ultrasound shows both the left arm (seen in the left side of the display), and the lower extremities (seen in the right side of the display). The white areas of the arm or legs is developing bone.
Ultrasound, normal fetus - arms and legs
illustration
Ultrasound, normal relaxed placenta - illustration
This is a normal fetal ultrasound performed at 19 weeks gestation. This ultrasound shows two interesting features. In the foreground, to the left and middle of the screen, you can see the placenta, following the curve of the uterus. In the background on the right, where the cross hair is pointing, you can see the face with all the facial features visible.
Ultrasound, normal relaxed placenta
illustration
Ultrasound, color - normal umbilical cord - illustration
This is a normal color Doppler ultrasound of the umbilical cord performed at 30 weeks gestation. The cord is the colored area in the middle of the screen, with the different blood vessels represented by different colors. There are normally three vessels in the cord, two arteries and one vein. The umbilical cord is connected to the placenta, located in the middle left of the image.
Ultrasound, color - normal umbilical cord
illustration
Placenta - illustration
The placenta supplies the fetus with the blood supply and nutrients necessary for survival.
Placenta
illustration





Cesarean section - illustration
1. The uterus is exposed through the abdominal wall, and an incision is made in the uterine covering. 2. The muscles of the uterus are separated, producing a hole for the delivery of the infant. 3. The infant is delivered through the opening in the uterine wall, after which, the uterus is stitched closed.
Cesarean section
illustration
Ultrasound in pregnancy - illustration
The ultrasound has become a standard procedure used during pregnancy. It can demonstrate fetal growth and can detect increasing numbers of conditions including meningomyelocele, congenital heart disease, kidney abnormalities, hydrocephalus, anencephaly, club feet, and other deformities. Ultrasound does not produce ionizing radiation and is considered a very safe procedure for both the mother and the fetus.
Ultrasound in pregnancy
illustration
Anatomy of a normal placenta - illustration
The placenta provides the fetus with oxygen and nutrients and takes away waste such as carbon dioxide via the umbilical cord.
Anatomy of a normal placenta
illustration
Placenta previa - illustration
Placenta previa is a condition of pregnancy when the placenta implants in the lower part of the uterus, partly or completely obstructing the cervical outlet to the vagina (birth canal).
Placenta previa
illustration
Placenta - illustration
In the placenta, nutrients, wastes, and gases are exchanged between the mothers blood and the babys blood.
Placenta
illustration
Ultrasound, normal fetus - arms and legs - illustration
This is a normal fetal ultrasound performed at 19 weeks gestation. This is the type of spilt-screen display you might see during an ultrasound, or if the technician prints a copy of the ultrasound for you. This ultrasound shows both the left arm (seen in the left side of the display), and the lower extremities (seen in the right side of the display). The white areas of the arm or legs is developing bone.
Ultrasound, normal fetus - arms and legs
illustration
Ultrasound, normal relaxed placenta - illustration
This is a normal fetal ultrasound performed at 19 weeks gestation. This ultrasound shows two interesting features. In the foreground, to the left and middle of the screen, you can see the placenta, following the curve of the uterus. In the background on the right, where the cross hair is pointing, you can see the face with all the facial features visible.
Ultrasound, normal relaxed placenta
illustration
Ultrasound, color - normal umbilical cord - illustration
This is a normal color Doppler ultrasound of the umbilical cord performed at 30 weeks gestation. The cord is the colored area in the middle of the screen, with the different blood vessels represented by different colors. There are normally three vessels in the cord, two arteries and one vein. The umbilical cord is connected to the placenta, located in the middle left of the image.
Ultrasound, color - normal umbilical cord
illustration
Placenta - illustration
The placenta supplies the fetus with the blood supply and nutrients necessary for survival.
Placenta
illustration
Review Date: 4/16/2024
Reviewed By: John D. Jacobson, MD, Professor Emeritus, Department of Obstetrics and Gynecology, Loma Linda University School of Medicine, Loma Linda, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.