Waldenstrom macroglobulinemia
Show Alternative Names
Waldenström macroglobulinemia
Macroglobulinemia - primary
Lymphoplasmacytic lymphoma
Monoclonal macroglobulinemia
Waldenström macroglobulinemia
Waldenström macroglobulinemia (WM) is a cancer of the B lymphocytes (a type of white blood cell). WM is associated with the overproduction of proteins called IgM antibodies.
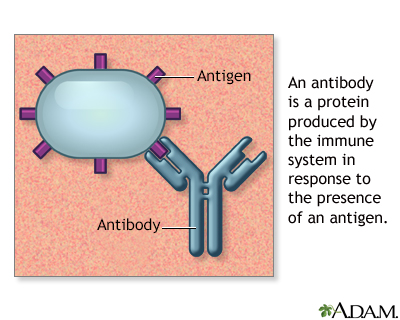
Antibodies
An antibody is a protein produced by the body's immune system when it detects harmful substances, called antigens. Examples of antigens include micr...

Image
Read Article Now
Book Mark Article
Causes
WM is a result of a condition called lymphoplasmacytic lymphoma. This is a cancer of the white blood cells, in which the B immune cells start dividing rapidly. The exact cause of too much production of the IgM antibody is unknown. Hepatitis C may increase the risk of WM. Gene mutations are often found in the malignant B cells.
Cancer
Cancer is the uncontrolled growth of abnormal cells in the body. Cancerous cells are also called malignant cells.
Read Article Now Book Mark ArticleProduction of excess IgM antibodies can cause several types of problems:
- Hyperviscosity, which causes the blood to become too thick. This can make it harder for blood to flow through small blood vessels.
- Neuropathy, or nerve damage, when the IgM antibody reacts with nerve tissue.
- Anemia, when the IgM antibody binds to red blood cells.
- Kidney disease, when the IgM antibody deposits in kidney tissue.
- Cryoglobulinemia and vasculitis (inflammation of the blood vessels) when the IgM antibody forms immune complexes with cold exposure.
Cryoglobulinemia
Cryoglobulinemia is the presence of abnormal proteins in the blood. These proteins thicken in cold temperatures.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
WM is very rare. Most people with this condition are over 65 years of age.
Symptoms
Symptoms of WM may include any of the following:
- Bleeding of the gums and nosebleeds
Bleeding of the gums
Bleeding gums can be a sign that you have or may develop gum disease. Ongoing gum bleeding may be due to plaque buildup on the teeth. It can also b...
Read Article Now Book Mark Article - Blurred or decreased vision
Blurred or decreased vision
There are many types of eye problems and vision disturbances, such as: Halos Blurred vision (the loss of sharpness of vision and the inability to see...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Bluish skin in the fingers after cold exposure
Bluish skin
A bluish color to the skin or mucous membrane is usually due to a lack of oxygen in the blood. The medical term is cyanosis.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Dizziness or confusion
Dizziness
Dizziness is a term that is often used to describe 2 different symptoms: lightheadedness and vertigo. Lightheadedness is a feeling that you might fai...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Easy bruising of the skin
- Fatigue
- Diarrhea
- Numbness, tingling, or burning pain in the hands, feet, fingers, toes, ears, or nose
Numbness
Numbness and tingling are abnormal sensations that can occur anywhere in your body, but they are often felt in your fingers, hands, feet, arms, or le...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Rash
Rash
Rashes involve changes in the color, feeling or texture of your skin.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Swollen glands
Swollen glands
Lymph nodes are present throughout your body. They are an important part of your immune system. Lymph nodes help your body recognize and fight germ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Unintentional weight loss
Unintentional weight loss
Unexplained weight loss is a decrease in body weight, when you did not try to lose the weight on your own. Many people gain and lose weight. Uninten...
Read Article Now Book Mark Article - Vision loss in one eye
Vision loss
There are many types of eye problems and vision disturbances, such as: Halos Blurred vision (the loss of sharpness of vision and the inability to see...
ImageRead Article Now Book Mark Article
Exams and Tests
A physical examination may reveal a swollen spleen, liver, and lymph nodes. An eye exam may show enlarged veins in the retina or retinal bleeding (hemorrhages).
Swollen spleen
Splenomegaly is a larger-than-normal spleen. The spleen is an organ in the upper left part of the belly.

Image
Read Article Now
Book Mark Article
A CBC may show a low number of red blood cells or platelets. Blood chemistry may show evidence of kidney disease.
CBC
A complete blood count (CBC) test measures the following:The number of white blood cells (WBC count)The number of red blood cells (RBC count)The numb...

Image
Read Article Now
Book Mark Article
Blood chemistry
A comprehensive metabolic panel is a group of blood tests. They provide an overall picture of your body's chemical balance and metabolism. Metaboli...

Image
Read Article Now
Book Mark Article
A test called serum protein electrophoresis shows an increased level of the IgM antibody. Levels are often higher than 300 milligrams per deciliter (mg/dL), or 3000 mg/L. An immunofixation test will be done to show that the IgM antibody is derived from a single cell type (clonal).
Serum protein electrophoresis
This lab test measures the types of protein in the fluid (serum) part of a blood sample. This fluid is called serum.
Image
Read Article Now
Book Mark Article
A serum viscosity test can tell if the blood has become thick. Symptoms usually occur when the blood is four times thicker than normal.
A bone marrow biopsy will show increased numbers of abnormal cells that look like both lymphocytes and plasma cells.
Additional tests that may be done include:
- 24-hour urine protein
Urine protein
The urine protein dipstick test measures the presence of all proteins, including albumin, in a urine sample. Albumin and protein can also be measured...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Total protein
Total protein
The total protein test measures the total amount of two classes of proteins found in the fluid portion of your blood. These are albumin and globulin...
ImageRead Article Now Book Mark Article - Immunofixation in urine
Immunofixation in urine
Urine immunofixation is a test to look for abnormal proteins in urine.
Read Article Now Book Mark Article - T (thymus derived) lymphocyte count
T (thymus derived) lymphocyte count
A T-cell count measures the number of T cells in the blood. Your health care provider may order this test if you have signs of a weak immune system,...
ImageRead Article Now Book Mark Article - Bone x-rays
Treatment
Some people with WM who have increased IgM antibodies do not have symptoms. This condition is known as smoldering WM. No treatment is needed other than careful follow-up.
In people with symptoms, treatment aims at decreasing the symptoms and the risk of developing organ damage. There is no current standard treatment. Your health care provider may suggest that you participate in a clinical trial.
Plasmapheresis removes IgM antibodies from the blood. It also controls the symptoms caused by blood thickening.
Medicines may include corticosteroids, a combination of chemotherapy medicines and the monoclonal antibody to B cells, rituximab.
Autologous stem cell transplant may be recommended for some people with otherwise good health.
People who have a low number of red or white blood cells or platelets may need transfusions or antibiotics.
Outlook (Prognosis)
The average survival is about 5 years. Some people live more than 10 years.
In some people, the disorder may produce few symptoms and progress slowly.
Possible Complications
Complications of WM may include:
- Changes in mental function, possibly leading to coma
Coma
Decreased alertness is a state of reduced awareness and is often a serious condition. A coma is the most severe state of decreased alertness from whi...
Read Article Now Book Mark Article - Heart failure
Heart failure
Heart failure is a condition in which the heart is no longer able to pump oxygen-rich blood to the rest of the body efficiently. This causes symptom...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Gastrointestinal bleeding or malabsorption
- Vision problems
Vision problems
There are many types of eye problems and vision disturbances, such as: Halos Blurred vision (the loss of sharpness of vision and the inability to see...
ImageRead Article Now Book Mark Article - Hives
Hives
Hives are raised, often itchy, red bumps (welts) on the surface of the skin. They can be an allergic reaction to food or medicine. They can also ap...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
When to Contact a Medical Professional
Contact your provider if symptoms of WM develop.
Review Date:
4/19/2022
Reviewed By
Diane M. Horowitz, MD, Rheumatology and Internal Medicine, Northwell Health, Great Neck, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
References
Kapoor P, Ansell SM, Fonseca R, et al. Diagnosis and management of Waldenström macroglobulinemia: Mayo stratification of macroglobulinemia and risk-adapted therapy (mSMART) guidelines 2016. JAMA Oncol. 2017;3(9):1257-1265. PMID: 28056114 pubmed.ncbi.nlm.nih.gov/28056114/.
Rajkumar SV. Plasma cell disorders. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier; 2020:chap 178.
Treon SP, Castillo JJ, Hunter ZR, Merlini G. Waldenström macroglobulinemia/lymphoplasmacytic lymphoma. In: Hoffman R, Benz EJ, Silberstein LE, et al, eds. Hematology: Basic Principles and Practice. 7th ed. Philadelphia, PA: Elsevier; 2018:chap 87.
Disclaimer
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites.
No warranty of any kind, either expressed or implied, is made as to the accuracy, reliability, timeliness, or correctness of any translations made by a third-party service of the information provided herein into any other language. © 1997-
A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.

 All rights reserved.
All rights reserved.