Hypogonadotropic hypogonadism
Hypogonadism is a condition in which the male testes or the female ovaries produce little or no sex hormones.
Hypogonadism
Hypogonadism occurs when the body's sex glands (gonads) produce little or no hormones. In men, these glands are the testes. In women, these glands ...

Testes
The testes are 2 egg-shaped male reproductive organs located in the scrotum. They produce sperm and the male hormone, testosterone.

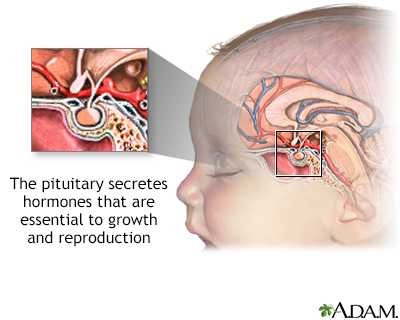
Hypogonadotropic hypogonadism (HH) is a form of hypogonadism that is due to a problem with the pituitary gland or hypothalamus.
Causes
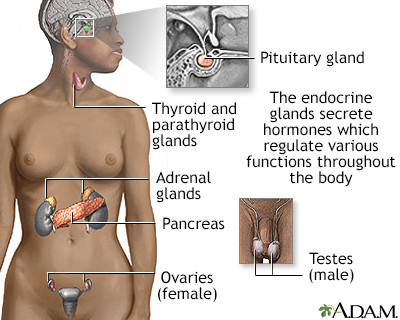
HH is caused by a lack of hormones that normally stimulate the ovaries or testes. These hormones include:
- Gonadotropin-releasing hormone (GnRH)
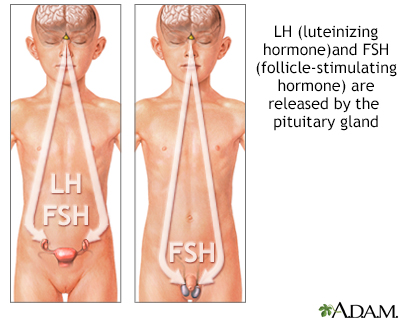
- Follicle stimulating hormone (FSH)
- Luteinizing hormone (LH)
Normally:
- The hypothalamus in the brain releases GnRH.
- This hormone stimulates the pituitary gland to release FSH and LH.
- These hormones tell the female ovaries or the male testes to release hormones that lead to normal sexual development in puberty, normal menstrual cycles, estrogen levels and fertility in adult women, and normal testosterone production and sperm production in adult men.
- Any change in this hormone release chain causes a lack of sex hormones. This prevents normal sexual maturity in children and normal function of the testicles or ovaries in adults.
There are several causes of HH:
- Damage to the pituitary gland or hypothalamus from surgery, injury, tumor, infection, or radiation
- Genetic defects
- High doses or long-term use of opioid or steroid (glucocorticoid) medicines
- High prolactin level (a different hormone released by the pituitary)
- Severe stress
- Nutritional problems (both rapid weight gain or weight loss)
- Long-term (chronic) medical diseases, including chronic inflammation or infections
- Drug use, such as heroin or use or abuse of prescription opioid medicines
- Certain medical conditions, such as iron overload
Iron overload
Hemochromatosis is a condition in which there is too much iron in the body. It is also called iron overload.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Kallmann syndrome is an inherited form of HH. Some people with this condition also lose their sense of smell (anosmia).
Symptoms
Children:
- Lack of growth and sexual development at the standard age for puberty (development may be very late or incomplete)
- In girls, a lack of breast development and menstrual periods
- In boys, no development of sex characteristics, such as enlargement of the testes and penis, deepening of the voice, and facial hair
- Inability to smell (in some cases)
- Short stature (in some cases)
Short stature
A child who has short stature is much shorter than children who are the same age and sex. Your health care provider will go over your child's growth ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Adults:
- Loss of interest in sex (libido) in men
- Loss of menstrual periods (amenorrhea) in women
- Decreased energy and interest in activities
- Loss of muscle mass in men
- Weight gain
- Mood changes
- Infertility
Infertility
Infertility means you cannot get pregnant (conceive). There are 2 types of infertility:Primary infertility refers to couples who have not become preg...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Exams and Tests
Your health care provider will perform a physical exam and ask about your symptoms.
Tests that may be done include:
- Blood tests to measure hormone levels such as FSH, LH, TSH, prolactin, testosterone and estradiol
- LH response to GnRH
LH response to GnRH
LH response to GnRH is a blood test to help determine if your pituitary gland can correctly respond to gonadotropin releasing hormone (GnRH). LH sta...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - MRI of the pituitary gland/hypothalamus (to look for a tumor or other growth)
MRI
A magnetic resonance imaging (MRI) scan is an imaging test that uses powerful magnets and radio waves to create pictures of the body. It does not us...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Genetic testing
- Blood tests to check for iron saturation level
Treatment
Treatment depends on the source of the problem, but may involve:
- Injections of testosterone (in males)
Testosterone
A testosterone test measures the amount of the male hormone, testosterone, in the blood. Both men and women produce this hormone. The test described...
ImageRead Article Now Book Mark Article - Slow-release testosterone skin patch (in males)
- Testosterone gels (in males)
- Estrogen and progesterone pills or skin patches (in females)
- GnRH injections
- HCG injections
Outlook (Prognosis)
The right hormone treatment will cause puberty to start in children and may restore fertility in adults. If the condition begins after puberty or in adulthood, symptoms will often improve with treatment.
Possible Complications
Health problems that may result from HH include:
- Delayed puberty
- Early menopause (in females)
- Infertility
- Low bone density and fractures later in life
- Low self-esteem due to late start of puberty (emotional support may be helpful)
- Sexual problems, such as low libido
When to Contact a Medical Professional
Contact your provider if:
- Your child does not start puberty at the appropriate time.
- You are a woman under age 40 and your menstrual cycles stop.
- You have lost armpit or pubic hair.
- You are a man and you have decreased interest in sex.
Reviewed By
Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
Bhasin S, Brito JP, Cunningham GR, et al. Testosterone therapy in men with hypogonadism: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2018;103(5):1715-1744. PMID: 29562364 pubmed.ncbi.nlm.nih.gov/29562364/.
Styne DM. Physiology and disorders of puberty. In: Melmed S, Auchus RJ, Goldfine AB, Koenig RJ, Rosen CJ, eds. Williams Textbook of Endocrinology. 14th ed. Philadelphia, PA: Elsevier; 2020:chap 26.
White PC. Sexual development. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 220.
 All rights reserved.
All rights reserved.