Acromegaly
Acromegaly is a condition in which there is too much growth hormone (GH) in your body.
Causes
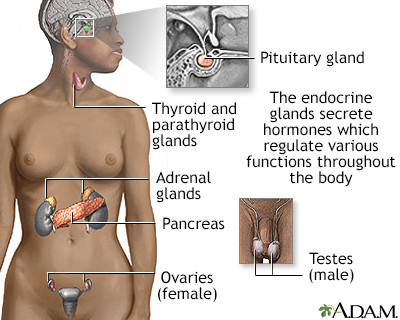
Acromegaly is a rare condition. It is caused when the pituitary gland makes too much GH. The pituitary gland is a small endocrine gland attached to the bottom of the brain. It controls, makes, and releases several hormones, including GH.
Endocrine gland
Endocrine glands release (secrete) hormones into the bloodstream. The endocrine glands include:AdrenalHypothalamusIslets of Langerhans in the pancrea...

Usually, a noncancerous (benign) tumor of the pituitary gland releases too much GH. In rare cases, pituitary tumors can be inherited.
In children, too much GH causes gigantism rather than acromegaly.
Gigantism
Gigantism is abnormal growth due to an excess of growth hormone (GH) during childhood.
Symptoms
Symptoms of acromegaly may include any of the following:
- Body odor
- Blood in the stool
- Carpal tunnel syndrome
Carpal tunnel syndrome
Carpal tunnel syndrome is a condition in which there is excessive pressure on the median nerve at the wrist. This is the nerve that allows feeling a...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Decreased muscle strength (weakness)
- Decreased peripheral vision
- Dental problems, gaps between the teeth
- Easy fatigue
Fatigue
Fatigue is a feeling of weariness, tiredness, or lack of energy.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Enlarged tongue
- Excessive height (when excess GH production begins in childhood)
- Excessive sweating
- Headache
- Heart enlargement, which can cause fainting or shortness of breath
- Hoarseness
Hoarseness
Hoarseness refers to difficulty making sounds when trying to speak. Vocal sounds may be weak, breathy, scratchy, or husky, and the pitch or quality ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Jaw pain
- Joint pain, limited joint movement, swelling of the bony areas around a joint
- Large bones of the face, large jaw and tongue, widely spaced teeth
- Large feet (change in shoe size), large hands (change in ring or glove size)
- Large glands in the skin (sebaceous glands) causing oily skin, thickening of the skin, skin tags (growths)
- Sleep apnea
Sleep apnea
Obstructive sleep apnea (OSA) is a problem in which your breathing pauses during sleep. This occurs because of narrowed or blocked airways.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Widened fingers or toes, with swelling, redness, and pain


Other symptoms that may occur with this disease:
- Colon polyps
Colon polyps
A colorectal polyp is a growth on the lining of the colon or rectum.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Excess hair growth in females (hirsutism)
Hirsutism
Most of the time, women have fine hair above their lips and on their chin, chest, abdomen, or back. The growth of coarse dark hair in these areas (m...
Read Article Now Book Mark Article - High blood pressure
- Type 2 diabetes
- Thyroid enlargement
- Weight gain
Exams and Tests
Your health care provider will perform a physical exam and ask about your symptoms.
The following tests may be ordered to confirm the diagnosis of acromegaly and check for complications:
- Blood glucose
Blood glucose
A blood sugar test measures the amount of sugar (glucose) in a sample of your blood. Glucose is a major source of energy for most cells of the body, ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Growth hormone
Growth hormone
The growth hormone test measures the amount of growth hormone in the blood. The pituitary gland makes growth hormone, which causes a child to grow. ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Insulin-like growth factor 1 (IGF-1)
- Prolactin
Prolactin
Prolactin is a hormone released by the pituitary gland. The prolactin blood test measures the amount of prolactin in the blood.
ImageRead Article Now Book Mark Article - Spine x-ray
Spine x-ray
A thoracic spine x-ray is an x-ray of the 12 chest (thoracic) bones (vertebrae) of the spine. The vertebrae are separated by flat pads of cartilage ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - MRI of the brain, including the pituitary gland
MRI of the brain
A head MRI (magnetic resonance imaging) is an imaging test that uses powerful magnets and radio waves to create pictures of the brain and surrounding...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Echocardiogram
Echocardiogram
An echocardiogram is a test that uses sound waves to create pictures of the heart. The picture and information it produces is more detailed than a s...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Colonoscopy
Colonoscopy
A colonoscopy is an exam that views the inside of the colon (large intestine) and rectum, using a tool called a colonoscope. The colonoscope has a sm...
ImageRead Article Now Book Mark Article - Sleep study
Other tests may be ordered to check whether the rest of the pituitary gland is working normally.
Often a GH suppression test is needed. This involves drawing blood from a vein 4 or 5 times over 2 hours before and after drinking a specific amount of a sugar solution. Glucose and GH are measured in the blood.
GH suppression test
The growth hormone suppression test determines whether growth hormone (GH) production can be suppressed by taking a specific amount of glucose (calle...
Treatment
Surgery to remove the pituitary tumor that is causing this condition often corrects the abnormal GH. Sometimes, the tumor is too large to be removed completely and acromegaly is not cured. In this case, medicines and radiation (radiotherapy) may be used to treat acromegaly.
Radiation
Radiation therapy uses high-powered radiation (such as x-rays or gamma rays), particles, or radioactive seeds to kill cancer cells.

Some people with tumors that are too complicated to remove by surgery are treated with medicines instead of surgery. These medicines may block the production of GH from the pituitary gland or prevent the action of GH in other parts of the body.
After treatment, you will need to see your provider regularly to make sure that the pituitary gland is working normally and that acromegaly does not come back. Yearly evaluations are usually recommended.
Support Groups
More information and support for people with acromegaly and their families can be found at:
- National Institute of Diabetes and Digestive and Kidney Diseases -- www.niddk.nih.gov/health-information/endocrine-diseases/acromegaly
- National Organization for Rare Disorders -- rarediseases.org/rare-diseases/acromegaly/
Outlook (Prognosis)
Pituitary surgery is successful in most people, depending on the size of the tumor and the experience of the neurosurgeon with pituitary tumors.
Tumor
A tumor is an abnormal growth of body tissue. Tumors can be cancerous (malignant) or noncancerous (benign).
Read Article Now Book Mark ArticleWithout treatment, the symptoms will get worse. Conditions such as high blood pressure, diabetes, and heart disease may result.
When to Contact a Medical Professional
Contact your provider if:
- You have symptoms of acromegaly
- Your symptoms do not improve with treatment
Prevention
Acromegaly cannot be prevented. Early treatment may prevent the disease from getting worse and help to avoid complications.
Reviewed By
Sandeep K. Dhaliwal, MD, board-certified in Diabetes, Endocrinology, and Metabolism, Springfield, VA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
Biondi B. Endocrine disorders and cardiovascular disease. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 96.
James WD, Elston DM, Treat JR, Rosenbach MA, Neuhaus IM. Endocrine diseases. In: James WD, Elston DM, Treat JR, Rosenbach MA, Neuhaus IM, eds. Andrews' Diseases of the Skin: Clinical Dermatology. 13th ed. Philadelphia, PA: Elsevier; 2020:chap 24.
Katznelson L, Laws ER Jr, Melmed S, et al. Acromegaly: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2014;99(11):3933-3951. PMID: 25356808 pubmed.ncbi.nlm.nih.gov/25356808/.
Lebovitz HE. Hyperglycemia Secondary to Non-Traditional Diabetic Conditions. In: Robertson RP, ed. DeGroot's Endocrinology. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 35.
 All rights reserved.
All rights reserved.