

Acute respiratory distress syndrome
Noncardiogenic pulmonary edema; Increased-permeability pulmonary edema; ARDS; Acute lung injuryAcute respiratory distress syndrome (ARDS) is a life-threatening lung condition that prevents enough oxygen from getting to the lungs and into the blood. Infants can also have respiratory distress syndrome.
Respiratory distress syndrome
Neonatal respiratory distress syndrome (RDS) is a problem often seen in premature babies. The condition makes it hard for the baby to breathe....
Read Article Now Book Mark ArticleCauses
ARDS can be caused by any major direct or indirect injury to the lung. Common causes include:
- Breathing vomit into the lungs (aspiration)
Aspiration
Aspiration means to draw in or out using a sucking motion. It has two meanings:Breathing in a foreign object (for example, sucking food into the air...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Inhaling chemicals
- Lung transplant
-
Pneumonia, including COVID-19 infection
Pneumonia
Pneumonia is inflamed or swollen lung tissue due to infection with a germ. This article covers community-acquired pneumonia (CAP). This type of pneu...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Septic shock (infection throughout the body)
Septic shock
Septic shock is a serious condition that occurs when a body-wide infection leads to dangerously low blood pressure.
Read Article Now Book Mark Article - Transfusions (multiple)
- Trauma
Depending on the amount of oxygen in the blood and during breathing, the severity of ARDS is classified as:
- Mild
- Moderate
- Severe
ARDS leads to a buildup of fluid in the air sacs (alveoli). This fluid prevents enough oxygen from passing into the bloodstream.
The fluid buildup also makes the lungs heavy and stiff. This decreases the lungs' ability to expand. The level of oxygen in the blood can stay dangerously low, even if the person receives oxygen from a breathing machine (ventilator) through a breathing tube (endotracheal tube).
Ventilator
A ventilator is a machine that breathes for you or helps you breathe. It is also called a breathing machine or respirator. The ventilator: Is attac...
Read Article Now Book Mark ArticleARDS often occurs along with the failure of other organ systems, such as the heart, liver or kidneys. Cigarette smoking and heavy alcohol use may be risk factors for its development.
Kidneys
Acute kidney failure is the rapid (less than 2 days) loss of your kidneys' ability to remove waste and help balance fluids and electrolytes in your b...

Symptoms
Symptoms usually develop within 24 to 48 hours of the injury or illness. Often, people with ARDS are so sick they cannot report symptoms. Symptoms can include any of the following:
- Shortness of breath
- Fast heartbeat
- Low blood pressure and organ failure
- Rapid breathing
Exams and Tests
Listening to the chest with a stethoscope (auscultation) reveals abnormal breath sounds, such as crackles, which may be signs of fluid in the lungs. Often, blood pressure is low. Blue skin, lips, and nails caused by lack of oxygen to the tissues (cyanosis) is often seen.
Auscultation
Auscultation is listening to the sounds of the body during a physical examination.

Cyanosis
A bluish color to the skin or mucous membrane is usually due to a lack of oxygen in the blood. The medical term is cyanosis.

Tests used to diagnose ARDS include:
-
Arterial blood gas
Arterial blood gas
Blood gases are a measurement of how much oxygen and carbon dioxide are in your blood. They also determine the acidity (pH) of your blood.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Blood tests, including CBC (complete blood count) and blood chemistries
CBC
A complete blood count (CBC) test measures the following:The number of white blood cells (WBC count)The number of red blood cells (RBC count)The numb...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Blood and urine cultures
Blood
A blood culture is a laboratory test to check for bacteria or other germs in a blood sample.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleUrine
A urine culture is a lab test to check for bacteria or other germs in a urine sample. It can be used to check for a urinary tract infection in adults...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Bronchoscopy in some people
Bronchoscopy
Bronchoscopy is a test to view the airways and diagnose lung disease. It may also be used during the treatment of some lung conditions.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Chest x-ray or CT scan
Chest x-ray
A chest x-ray is an x-ray of the chest, lungs, heart, large arteries, ribs, and diaphragm.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Sputum cultures and analysis
Sputum cultures
Routine sputum culture is a laboratory test that looks for germs that cause infection. Sputum is the material that comes up from air passages when y...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Tests for possible infections
An echocardiogram may be needed to rule out heart failure, which can look similar to ARDS on a chest x-ray.
Echocardiogram
An echocardiogram is a test that uses sound waves to create pictures of the heart. The picture and information it produces is more detailed than a s...

Heart failure
Heart failure is a condition in which the heart is no longer able to pump oxygen-rich blood to the rest of the body efficiently. This causes symptom...

Treatment
ARDS often needs to be treated in an intensive care unit (ICU).
The goal of treatment is to provide breathing support and treat the cause of ARDS. This may involve medicines to treat infections, reduce inflammation, and remove fluid from the lungs.
A ventilator is used to deliver high doses of oxygen and positive pressure to the damaged lungs. People often need to be deeply sedated with medicines. During treatment, your health care providers make every effort to protect your lungs from further damage. Certain ways of using the ventilator can protect your lungs better and improve chances of recovery. Treatment is mainly supportive until the lungs recover.
Sometimes, a treatment called extracorporeal membrane oxygenation (ECMO) is done. During ECMO, blood is filtered through a machine to provide oxygen and remove carbon dioxide.
Support Groups
Many family members of people with ARDS are under extreme stress. They can often relieve this stress by joining support groups where members share common experiences and problems.
Support groups
The following organizations are good resources for information on lung disease:American Lung Association -- www. lung. orgNational Heart, Lung, and B...

Outlook (Prognosis)
About one third of people with ARDS die of the disease. Those who live often get back most of their normal lung function, but many people have permanent (usually mild) lung damage.
Many people who survive ARDS have memory loss or other quality-of-life problems after they recover. This is due to brain damage that occurred when the lungs were not working properly and the brain was not getting enough oxygen. Some people can also have post-traumatic stress after surviving ARDS.
Possible Complications
Problems that may result from ARDS or its treatment include:
- Failure of many organ systems
- Lung damage, such as a collapsed lung (also called pneumothorax) due to injury from the breathing machine needed to treat the disease
Pneumothorax
A collapsed lung occurs when air escapes from the lung. The air then fills the space outside of the lung between the lung and chest wall. This buil...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Pulmonary fibrosis (scarring of the lung)
Pulmonary fibrosis
Idiopathic pulmonary fibrosis (IPF) is scarring or thickening of the lungs without a known cause.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Ventilator-associated pneumonia
Ventilator-associated pneumonia
Hospital-acquired pneumonia is an infection of the lungs that occurs during a hospital stay. This type of pneumonia can be very severe. Sometimes, ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
When to Contact a Medical Professional
ARDS most often occurs during another illness, for which the person is already in the hospital. In some cases, a healthy person has severe pneumonia that gets worse and becomes ARDS. If you have trouble breathing, call your local emergency number (such as 911) or go to the emergency room.
References
Binnie A, Herridge MS, Lee WL. Acute respiratory distress syndrome. In: Broaddus VC, Ernst JD, King TE, et al, eds. Murray and Nadel's Textbook of Respiratory Medicine. 7th ed. Philadelphia, PA: Elsevier; 2022:chap 134.
Matthay MA, Ware LB. Acute respiratory failure. In: Goldman L, Cooney KA, eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier; 2024:chap 90.
Seigel TA, Johnson NJ. Mechanical ventilation and noninvasive ventilatory support. In: Walls RM, ed. Rosen's Emergency Medicine: Concepts and Clinical Practice. 10th ed. Philadelphia, PA: Elsevier; 2023:chap 2.
-
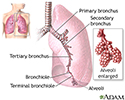
Lungs - illustration
The major features of the lungs include the bronchi, the bronchioles and the alveoli. The alveoli are the microscopic blood vessel-lined sacks in which oxygen and carbon dioxide gas are exchanged.
Lungs
illustration
-
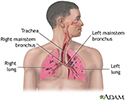
Respiratory system - illustration
Air is breathed in through the nasal passageways, travels through the trachea and bronchi to the lungs.
Respiratory system
illustration
-
Lungs - illustration
The major features of the lungs include the bronchi, the bronchioles and the alveoli. The alveoli are the microscopic blood vessel-lined sacks in which oxygen and carbon dioxide gas are exchanged.
Lungs
illustration
-
Respiratory system - illustration
Air is breathed in through the nasal passageways, travels through the trachea and bronchi to the lungs.
Respiratory system
illustration
-
Sinusitis - InDepth
(In-Depth)
-
Pneumonia - InDepth
(In-Depth)
-
Restless legs syndrome and related disorders - InDepth
(In-Depth)
-
Colds and the flu - InDepth
(In-Depth)
-
Travel to developing countries - InDepth
(In-Depth)
-
Cysteine
(Alt. Medicine)
-
Asthma in children and adolescents - InDepth
(In-Depth)
-
Insomnia - InDepth
(In-Depth)
-
Asthma in adults - InDepth
(In-Depth)
-
Anxiety disorders - InDepth
(In-Depth)
Review Date: 11/25/2023
Reviewed By: Denis Hadjiliadis, MD, MHS, Paul F. Harron, Jr. Professor of Medicine, Pulmonary, Allergy, and Critical Care, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.