
Radical prostatectomy - discharge
Prostatectomy - radical - discharge; Radical retropubic prostatectomy - discharge; Radical perineal prostatectomy - discharge; Laparoscopic radical prostatectomy - discharge; LRP - discharge; Robotic-assisted laparoscopic prostatectomy - discharge; RALP - discharge; Pelvic lymphadenectomy - discharge; Prostate cancer - prostatectomyYou had surgery to remove all of your prostate, some tissue near your prostate, and probably some lymph nodes. This article tells you how to take care of yourself at home after the surgery.
When You're in the Hospital
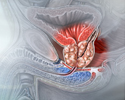
You had surgery to remove all of your prostate, some tissue near your prostate, and probably some lymph nodes. This was done to treat prostate cancer.
- Your surgeon may have made an incision (cut) either in the lower part of your belly or in the area between your scrotum and anus (open surgery).
- Your surgeon may have used a robot or a laparoscope (a thin tube with a tiny camera on the end). You will have several small incisions on your belly.
What to Expect at Home
You may be tired and need more rest for 3 to 4 weeks after you go home. You may have pain or discomfort in your belly or the area between your scrotum and anus for 2 to 3 weeks.
You will go home with a catheter (tube) to drain urine from your bladder. This will be removed after 1 to 3 weeks.
You may go home with an additional drain (called a Jackson-Pratt, or JP drain). You will be taught how to empty it and care for it.
Wound Care
Change the dressing over your surgical wound once a day, or sooner if it becomes soiled. Your health care provider will tell you when you do not need to keep your wound covered. Keep the wound area clean by washing it with mild soap and water.
- You may remove the wound dressings and take showers if sutures, staples, or glue were used to close your skin. Cover the incision with plastic wrap before showering for the first week if you have tape (Steri-Strips) over it.
- Do not soak in a bathtub or hot tub, or go swimming, as long as you have a catheter. You can do these activities after the catheter is removed and your surgeon has told you it is OK to do so.
Your scrotum may be swollen for 2 to 3 weeks if you had open surgery. You may need to wear either a support (like a jock strap) or brief underwear until the swelling goes away. While you are in bed, you may use a towel under your scrotum for support.
You may have a drain (called a Jackson-Pratt, or JP drain) below your belly button that helps extra fluid drain from your body and prevent it from building up in your body. Your provider will take it out after 1 to 3 days.
A drain (called a Jackson-Pratt, or JP ...
A closed suction drain is placed under your skin during surgery. This drain removes any blood or other fluids that might build up in this area....
Urinary Catheters
While you have a urinary catheter:
Urinary catheter
A urinary catheter is a tube placed in the body to drain and collect urine from the bladder.
- You may feel spasms in your bladder. Your provider can give you medicine for this.
- You will need to make sure your indwelling catheter is working properly. You will also need to know how to clean the tube and the area where it attaches to your body so that you do not get an infection or skin irritation.
- The urine in your drainage bag may be a darker red color. This is normal.
After your catheter is removed:
- You may have burning when you pee, blood in the urine, frequent urination, and an urgent need to urinate.
- You may have some urine leakage (incontinence). This should improve over time. You should have almost normal bladder control within 3 to 6 months.
- You will learn exercises (called Kegel exercises) that strengthen the muscles in your pelvis. You can do these exercises any time you are sitting or lying down.
Exercises (called Kegel exercises)
Kegel exercises can help make the muscles under the uterus, bladder, and bowel (large intestine) stronger. They can help both men and women who have...
Read Article Now Book Mark Article
Other Self-care
Do not drive the first 3 weeks after you come home. Avoid long car trips if you can. If you need to take a long car trip, stop at least every 2 hours.
Do not lift anything heavier than a 1-gallon (4 liters) milk jug for the first 6 weeks. You can slowly work back up to your normal exercise routine after that. You can do everyday activities around the house if you feel up to it. But expect to get tired more easily.
Drink at least 8 glasses of water a day, eat a lot of fruits and vegetables, and take stool softeners to prevent constipation. Do not strain during bowel movements.
For the first few weeks after surgery, take only the medicines your provider has told you to take.
- You may need to take antibiotics to help prevent infection.
- Check with your surgeon before taking aspirin, ibuprofen (Aleve, Motrin), naproxen (Aleve, Naprosyn), or any other drugs like these. They may cause problems with blood clots in your urine.
Sexual Problems After Surgery
Sexual problems you may notice are:
- Your erection may not be as rigid. Some men are not able to have an erection.
- Your orgasm may not be as intense or pleasurable as before.
- You may notice no semen at all when you have an orgasm.
These problems may get better or even go away, but it may take many months or more than a year. The lack of an ejaculate (semen coming out with orgasm) will be permanent. Ask your provider about medicines that will help.
When to Call the Doctor
Contact your provider if:
- You have pain in your belly that does not go away when you take your pain medicines
- It is hard to breathe
- You have a cough that does not go away
- You cannot drink or eat
- Your temperature is above 100.5°F (38°C)
- Your surgical cuts are bleeding, red, warm to the touch, or have a thick, yellow, green, or milky drainage
- You have signs of infection (burning sensation when you urinate, fever, or chills)
- Your urine stream is not as strong or you cannot pee at all
- You have pain, redness, or swelling in your legs
While you have a urinary catheter, call your provider if:
- You have pain near the catheter
- You are leaking urine
- You notice more blood in your urine
- Your catheter seems blocked
- You notice grit or stones in your urine
- Your urine smells bad, or it is cloudy or a different color
- Your catheter has fallen out
References
Nelson WG, Antonarakis ES, Carter HB, De Marzo AM, et al. Prostate cancer. In: Niederhuber JE, Armitage JO, Kastan MB, Doroshow JH, Tepper JE, eds. Abeloff's Clinical Oncology. 6th ed. Philadelphia, PA: Elsevier; 2020:chap 81.
Skolarus TA, Wolf AM, Erb NL, et al. American Cancer Society prostate cancer survivorship care guidelines. CA Cancer J Clin. 2014;64(4):225-249. PMID: 24916760 pubmed.ncbi.nlm.nih.gov/24916760/.
Taneja SS, Bjurlin MA. Active management strategies for localized prostate cancer. In: Partin AW, Domochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 153.
Review Date: 4/1/2023
Reviewed By: Kelly L. Stratton, MD, FACS, Associate Professor, Department of Urology, University of Oklahoma Health Sciences Center, Oklahoma City, OK. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.