
Hysterectomy - laparoscopic - discharge
Removal of the uterus - discharge; Laparoscopic hysterectomy - discharge; Total laparoscopic hysterectomy - discharge; TLH - discharge; Robotic assisted laparoscopic hysterectomy - dischargeYou were in the hospital to have surgery to remove your uterus. The fallopian tubes and ovaries may also have been removed. A laparoscope (a thin tube with a small camera on it) inserted through small cuts in your belly was used for the operation.
When You're in the Hospital
While you were in the hospital, you had surgery to remove your uterus. This is called a hysterectomy. The surgeon made 3 to 5 small cuts in your belly. A laparoscope (a thin tube with a small camera on it) and other small surgical tools were inserted through those incisions.
Part or all of your uterus was removed. Your fallopian tubes or ovaries may have also been taken out.
You probably spent 1 day in the hospital.
What to Expect at Home
It may take at least 4 to 6 weeks for you to feel completely better after your surgery. The first two weeks are most often the hardest. You may need to take pain medicine regularly.
Most people are able to stop taking pain medicine and increase their activity level after two weeks. Most people are able to perform more normal activities at this point, after two weeks such as desk work, office work, and light walking. In most cases, it takes 6 to 8 weeks for energy levels to return to normal.
If you had good sexual function before the surgery, you should continue to have good sexual function after you have completely healed. If you had problems with severe bleeding before your hysterectomy, sexual function often improves after surgery. If you have a decrease in your sexual function after your hysterectomy, talk with your health care provider about possible causes and treatments.
Activity
Start walking after surgery. Begin your everyday activities as soon as you feel up to it. Do not jog, do sit-ups, or play sports until you have checked with your surgeon.
Move around the house, shower, and use the stairs at home during the first week. If it hurts when you do something, stop doing that activity.
Ask your surgeon about driving. You may be able to drive after 2 or 3 days if you are not taking narcotic pain drugs.
You may lift 10 pounds or 4.5 kilograms (about the weight of a gallon or 4 liters of milk) or less. Do not do any heavy lifting or straining for the first 3 weeks. You may be able to go back to a desk job within a couple of weeks. But you may still get tired more easily at this time.
Do not put anything into your vagina for the first 8 to 12 weeks. This includes douching and tampons.
Do not have sexual intercourse for at least 12 weeks, and only after your surgeon says it is OK. Resuming intercourse sooner than that could lead to complications.
Wound Care
If sutures (stitches), staples, or glue were used to close your skin, you may remove your wound dressings (bandages) and take a shower the day after surgery.
If tape strips were used to close your skin, they should fall off on their own in about a week. If they are still in place after 10 days, remove them unless your surgeon tells you not to.
There may be sutures inside the vagina, where the cervix was attached before the surgery. The sutures will dissolve on their own in 8 to 12 weeks. Avoid inserting anything in the vaginal until your surgeon clears you after an exam.
Do not go swimming or soak in a bathtub or hot tub until your surgeon tells you it is OK.
Self-care
Try eating smaller meals than normal. Eat healthy snacks in between meals. Eat plenty of fruits and vegetables and drink at least 8 cups (2 liters) of water a day to keep from getting constipated.
Keep from getting constipated
Constipation is when you do not pass stool as often as you normally do. Your stool may become hard and dry, and it can be difficult to pass....

When to Call the Doctor
Contact your surgeon if:
- You have a fever above 100.5°F (38°C).
- Your surgical wound is bleeding, is red and warm to touch, or has thick, yellow, or green drainage.
- Your pain medicine is not helping your pain.
- It is hard to breathe.
- You have a cough that does not go away.
- You cannot drink or eat.
- You have nausea or vomiting.
- You are unable to pass any gas or have a bowel movement.
- You have pain or burning when you urinate, or you are unable to urinate.
- You have a discharge from your vagina that has a bad odor.
- You have bleeding from your vagina that is heavier than light spotting.
- You have a heavy, watery discharge from the vagina.
- You have swelling or redness in one of your legs.
References
American College of Obstetricians and Gynecologists website. Hysterectomy: frequently asked questions. www.acog.org/womens-health/faqs/hysterectomy. Updated September 2024. Accessed March 15, 2025.
Michener CM, Falcone T. Laparoscopic hysterectomy. In: Baggish MS, Karram MM, eds. Atlas of Pelvic Anatomy and Gynecologic Surgery. 5th ed. Philadelphia, PA: Elsevier; 2021:chap 114.
Prescott LS, Yunker AC, Alvarez R. Gynecologic surgery. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery. 21st ed. St Louis, MO: Elsevier; 2022:chap 71.
Raymond L, Lentz GM. Endoscopy in minimally invasive gynecologic surgery. In: Gershenson DM, Lentz GM, Valea FA, Lobo RA, eds. Comprehensive Gynecology. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 10.
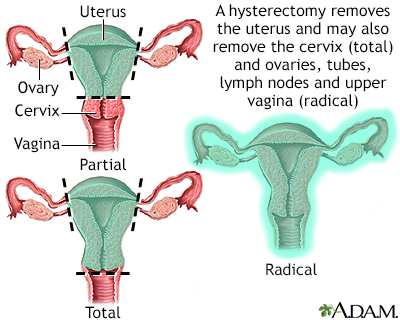
Hysterectomy - illustration
Hysterectomy is surgical removal of the uterus, resulting in inability to become pregnant. This surgery may be done for a variety of reasons including, but not restricted to, chronic pelvic inflammatory disease, uterine fibroids and cancer. A hysterectomy may be done through an abdominal or a vaginal incision.
Hysterectomy
illustration
Hysterectomy - illustration
Hysterectomy is surgical removal of the uterus, resulting in inability to become pregnant. This surgery may be done for a variety of reasons including, but not restricted to, chronic pelvic inflammatory disease, uterine fibroids and cancer. A hysterectomy may be done through an abdominal or a vaginal incision.
Hysterectomy
illustration
- Uterine fibroids and hysterectomy - InDepth(In-Depth)
- Cervical cancer - InDepth(In-Depth)
- Menstrual disorders - InDepth(In-Depth)
Review Date: 2/3/2025
Reviewed By: Peter J. Chen, MD, FACOG, Associate Professor of OBGYN at Cooper Medical School at Rowan University, Camden, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.