
Charcot foot
Charcot joint; Neuropathic arthropathy; Charcot neuropathic osteoarthropathy; Charcot arthropathy; Charcot osteoarthropathy; Diabetic Charcot footCharcot foot is a condition that affects the bones, joints, and soft tissue in the feet and ankles. It can develop as a result of nerve damage in the feet due to diabetes or other nerve injuries.
Causes
Charcot foot is a rare and disabling disorder. It is a result of nerve damage to the feet. A common cause is peripheral neuropathy.
Peripheral neuropathy
Peripheral nerves carry information to and from the brain. They also carry signals to and from the spinal cord to the rest of the body. Peripheral n...

Diabetes is the most common cause of this type of nerve damage. This damage is more common in people with type 1 diabetes. When blood sugar levels are high over a long time, both nerve and blood vessel damage occurs in the arms and legs.
Nerve damage makes it harder to notice the amount of pressure on the foot or if it is being stressed. The result is ongoing small injuries to the bones and ligaments that support the foot.
- You may develop bone stress fractures in your feet, yet never know it.
- Continuing to walk on the fractured bone often leads to further bone and joint damage.
Other factors leading to foot damage include:
- Blood vessel damage from diabetes can increase or change blood flow to the feet. This can lead to bone loss. Weakened bones in the feet increase the risk of fracture.
- Injury to the foot signals the body to produce more inflammation-causing chemicals. This contributes to swelling and bone loss.
Symptoms
Early foot symptoms may include:
- Mild pain and discomfort
- Redness
- Swelling
- Warmth in the affected foot (noticeably warmer than the other foot)
At later stages, bones in the foot break and move out of place, causing the foot or ankle to become deformed.
- A classic sign of Charcot is rocker-bottom foot. This occurs when the bones in middle of the foot collapse. This causes the arch of the foot to collapse and bow downward.
- The toes may curl downward.
Bones that stick out at odd angles can lead to pressure sores and foot ulcers.
Foot ulcers
If you have diabetes, you have an increased chance of developing foot sores, or ulcers, also called diabetic ulcers. Foot ulcers are a common reason ...
- Because the feet are numb, these sores and ulcers may grow wider or deeper before they are noticed.
- High blood sugar also makes it hard for the body to fight infection. As a result, these foot ulcers may become infected.
Exams and Tests
Charcot foot is not always easy to diagnose early on. It can be mistaken for sprains, bone infection, arthritis or joint swelling. Your health care provider will take your medical history and examine your foot and ankle.
Blood tests and other lab work may be done to help rule out other causes.
Your provider may check for nerve damage with these tests:
-
Electromyography
Electromyography
Electromyography (EMG) is a test that checks the health of the muscles and the nerves that control the muscles.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Nerve conduction velocity tests
Nerve conduction velocity tests
Nerve conduction velocity (NCV) is a test to see how fast electrical signals move through a nerve. This test is done along with electromyography (EM...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Nerve biopsy
Nerve biopsy
A nerve biopsy is the removal of a small piece of a nerve for examination.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
The following tests may be done to check for bone and joint damage:
-
Foot x-rays
x-rays
X-rays are a type of electromagnetic radiation, just like visible light. An x-ray machine sends individual x-ray waves through the body. The images...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
MRI
MRI
A leg MRI (magnetic resonance imaging) scan of the leg uses strong magnets to create pictures of the leg. This may include the ankle, foot, and surr...
Read Article Now Book Mark Article -
Bone scan
Bone scan
A bone scan is an imaging test used to diagnose bone diseases and find out how severe they are.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Foot x-rays may look normal at early stages of the condition. Diagnosis often comes down to recognizing early symptoms of Charcot foot: swelling, redness, and warmth of the affected foot.
Treatment
The goal of treatment is to stop bone loss, allow bones to heal, and prevent bones from moving out of place (deformity).
Immobilization -- Your provider will have you wear a total contact cast. This will help limit movement of your foot and ankle. You will likely be asked to keep your weight off your foot entirely, so you will need to use crutches, a knee-walker device, or wheelchair.
You will have new casts placed on your foot as the swelling comes down. Healing can take a couple of months or more.
Protective footwear -- Once your foot has healed, your provider may suggest footwear to help support your foot and prevent re-injury. These may include:
- Splints
- Braces
- Orthotic insoles
- Charcot restraint orthotic walker, a special boot that provides even pressure to the whole foot
Activity changes -- You will always be at risk for Charcot foot coming back or developing in your other foot. So your provider may recommend activity changes, such as limiting your standing or walking, to protect your feet. You may need to use a wheelchair to limit activity on your feet.
Surgery -- You may need surgery if you have foot ulcers that keep coming back or severe foot or ankle deformity. Surgery can help stabilize your foot and ankle joints and remove bony areas to prevent foot ulcers.
Ongoing monitoring -- You will need to see your provider for checkups and take steps to protect your feet for the rest of your life.
Outlook (Prognosis)
The prognosis depends on the severity of foot deformity and how well you heal without infection. Many people do well with braces, activity changes, and ongoing monitoring.
Possible Complications
Severe deformity of the foot increases the risk of foot ulcers. If ulcers or the underlying bone becomes infected and hard to treat, it may require amputation.
Amputation
Leg or foot amputation is the removal of a leg, foot or toes from the body. These body parts are called extremities. Amputations are done either by...
When to Contact a Medical Professional
Contact your provider if you have diabetes and your foot is warm, red, or swollen.
Prevention
Healthy habits can help prevent or delay Charcot foot:
- Keep good control of your blood glucose levels to help prevent or delay Charcot foot. But it can still occur, even in people with good diabetes control.
-
Take care of your feet. Check them every day.
Take care of your feet
Diabetes can damage the nerves and blood vessels in your feet. This damage can cause numbness and reduce feeling in your feet. As a result, your fe...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - See your foot doctor regularly.
- Check your feet regularly to look for cuts, redness and sores.
- Avoid injuring your feet.
References
Baxi O, Yeranosian M, Lin A, Munoz M, Lin S. Orthotic management of neuropathic and dysvascular feet. In: Webster JB, Murphy DP, eds. Atlas of Orthoses and Assistive Devices. 5th ed. Philadelphia, PA: Elsevier; 2019:chap 26.
Brownlee M, Aiello LP, Sun JK, et al. Complications of diabetes mellitus. In: Melmed S, Auchus RJ, Goldfine AB, Koenig RJ, Rosen CJ, eds. Williams Textbook of Endocrinology. 14th ed. Philadelphia, PA: Elsevier; 2020:chap 37.
ElSayed NA, Aleppo G, Aroda VR, et al, on behalf of the American Diabetes Association. 12. Retinopathy, Neuropathy, and Foot Care: Standards of Care in Diabetes-2023. Diabetes Care. 2023 1;46(Suppl 1):S203-S215. PMID: 36507636; PMCID: PMC9810462. pubmed.ncbi.nlm.nih.gov/36507636/.
-
Diabetes
Animation
-
Nerve conduction test - illustration
The nerve conduction velocity test is performed to evaluate nerve function. It tests the speed impulses travel through a nerve.
Nerve conduction test
illustration
-
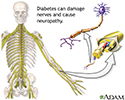
Diabetes and nerve damage - illustration
Diabetes can damage the nerves and cause a complication called neuropathy. This generally begins as loss of sensation in the toes, and possibly fingers. Eventually, the neuropathy can move up the person's legs or arms. Nerve damage results in decreased ability to feel pain, pressure, and extremes of temperature.
Diabetes and nerve damage
illustration
-
Diabetic foot care - illustration
People with diabetes are prone to foot problems because the disease can cause damage to the blood vessels and nerves, which may result in decreased ability to sense a trauma to the foot. The immune system is also altered, so that the person with diabetes cannot efficiently fight infection.
Diabetic foot care
illustration


-
Nerve conduction test - illustration
The nerve conduction velocity test is performed to evaluate nerve function. It tests the speed impulses travel through a nerve.
Nerve conduction test
illustration
-
Diabetes and nerve damage - illustration
Diabetes can damage the nerves and cause a complication called neuropathy. This generally begins as loss of sensation in the toes, and possibly fingers. Eventually, the neuropathy can move up the person's legs or arms. Nerve damage results in decreased ability to feel pain, pressure, and extremes of temperature.
Diabetes and nerve damage
illustration
-
Diabetic foot care - illustration
People with diabetes are prone to foot problems because the disease can cause damage to the blood vessels and nerves, which may result in decreased ability to sense a trauma to the foot. The immune system is also altered, so that the person with diabetes cannot efficiently fight infection.
Diabetic foot care
illustration
Review Date: 12/12/2022
Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.