

Osteomyelitis in children
Bone infection - children; Infection - bone - childrenOsteomyelitis is a bone infection caused by bacteria or other germs.
Causes
A bone infection is most often caused by bacteria. It can also be caused by fungi or other germs. In children, the long bones of the arms or legs are most often involved.
Long bones
Long bones are hard, dense bones that provide strength, structure, and mobility. The thigh bone (femur) is a long bone. A long bone has a shaft and...

When a child has osteomyelitis:
- Bacteria or other germs may spread to the bone from infected skin, muscles, or tendons next to the bone. This may occur under a skin sore.
- The infection can start in another part of the body and spread through the blood to the bone.
- The infection can be caused by an injury that breaks the skin and bone (open fracture). Bacteria can enter the skin and infect the bone.
Fracture
If more pressure is put on a bone than it can stand, it will split or break. A break of any size is called a fracture. If the broken bone punctures...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - The infection can also start after bone surgery. This is more likely if the surgery is done after an injury, or if metal rods or plates are placed in the bone.
Other risk factors include:
- Premature birth or delivery complications in newborns
- Diabetes
Diabetes
Diabetes is a long-term (chronic) disease in which the body cannot regulate the amount of sugar in the blood.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Poor blood supply
- Recent injury
- Sickle cell disease
Sickle cell disease
Sickle cell disease is a disorder passed down through families. The red blood cells that are normally shaped like a disk take on a sickle or crescen...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Infection due to a foreign body
- Pressure ulcers
Pressure ulcers
Pressure ulcers are also called bedsores, or pressure sores. They can form when your skin and soft tissue press against a harder surface, such as a ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Human bites or animal bites
Human bites
A human bite can break, puncture, or tear the skin. Bites that break the skin put you at risk for infection.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleAnimal bites
An animal bite can break, puncture, or tear the skin. Bites that break the skin put you at risk for infections.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Weakened immune system
Symptoms
Osteomyelitis symptoms include:
- Bone pain
Bone pain
Bone pain or tenderness is aching or other discomfort in one or more bones.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Excessive sweating
- Fever and chills
- General discomfort, uneasiness, or ill feeling (malaise)
Malaise
Malaise is a general feeling of discomfort, illness, or lack of well-being.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Local swelling, redness, and warmth
Swelling
Swelling is the enlargement of organs, skin, or other body parts. It is caused by a buildup of fluid in the tissues. The extra fluid can lead to a ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Pain at the infection site
- Swelling of the ankles, feet, and legs
Swelling of the ankles, feet, and legs
Painless swelling of the feet and ankles is a common problem, especially among older people. Abnormal buildup of fluid in the ankles, feet, and legs ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Refusing to walk (when leg bones are involved)
Infants with osteomyelitis may not have a fever or other signs of illness. They might avoid moving the infected limb due to pain.
Exams and Tests
Your child's health care provider will perform a physical exam and ask about the symptoms your child is having.
Tests that your child's provider may order include:
- Blood cultures
Blood cultures
A blood culture is a laboratory test to check for bacteria or other germs in a blood sample.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Bone biopsy (the sample is cultured and examined under a microscope)
Bone biopsy
A bone lesion biopsy is the removal of a piece of bone or bone marrow for examination.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Bone scan
Bone scan
A bone scan is an imaging test used to diagnose bone diseases and find out how severe they are.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Bone x-ray
Bone x-ray
A bone x-ray is an imaging test to look at the bones.
ImageRead Article Now Book Mark Article - Complete blood count (CBC)
Complete blood count
A complete blood count (CBC) test measures the following:The number of white blood cells (WBC count)The number of red blood cells (RBC count)The numb...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - C-reactive protein (CRP)
C-reactive protein (CRP)
C-reactive protein (CRP) is produced by the liver. The level of CRP rises when there is inflammation in the body. It is one of a group of proteins,...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Erythrocyte sedimentation rate (ESR)
Erythrocyte sedimentation rate (ESR)
ESR stands for erythrocyte sedimentation rate. It is commonly called a "sed rate. "It is a test that indirectly measures the level of certain protei...
ImageRead Article Now Book Mark Article - MRI of the bone
MRI
A magnetic resonance imaging (MRI) scan is an imaging test that uses powerful magnets and radio waves to create pictures of the body. It does not us...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Needle aspiration of the area of the affected bones
Needle aspiration
Aspiration means to draw in or out using a sucking motion. It has two meanings:Breathing in a foreign object (for example, sucking food into the air...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Treatment
The goal of treatment is to stop the infection and reduce damage to the bone and surrounding tissues.
Antibiotics are given to destroy the bacteria causing the infection:
- Your child may receive more than one antibiotic at a time.
- Antibiotics are taken for at least 4 to 6 weeks, often at home through an IV (intravenously, meaning through a vein). At some point, your child's provider may switch the medicine to antibiotic pills.
At home through an IV
You or your child will be going home from the hospital soon. Your health care provider has prescribed medicines or other treatments that you or your...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Surgery may be needed to remove dead bone tissue if the child has an infection that does not go away.
- If there are metal plates near the infection, they may need to be removed.
- The open space left by the removed bone tissue may be filled with bone graft or packing material. This promotes the growth of new bone tissue.
Bone graft
A bone graft is surgery to place new bone or bone substitutes into spaces around a broken bone or bone defects to stimulate healing.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
If your child was treated in the hospital for osteomyelitis, be sure to follow your provider's instructions on how to care for your child at home.
Outlook (Prognosis)
With treatment, the outcome for acute osteomyelitis is usually good.
The outlook is worse for those with long-term (chronic) osteomyelitis. Symptoms may come and go for years, even with surgery.
Chronic
Chronic refers to something that continues over an extended period of time. A chronic condition is usually long-lasting and does not easily or quick...

When to Contact a Medical Professional
Contact your child's provider if:
- Your child develops symptoms of osteomyelitis
- Your child has osteomyelitis and the symptoms continue, even with treatment
References
Dabov GD. Osteomyelitis. In: Azar FM, Beaty JH, Canale ST, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 21.
Krogstad P. Osteomyelitis. In: Cherry JD, Harrison GJ, Kaplan SL, Steinbach WJ, Hotez PJ, eds. Feigin and Cherry's Textbook of Pediatric Infectious Diseases. 8th ed. Philadelphia, PA: Elsevier; 2019:chap 55.
Robinette E, Shah SS. Osteomyelitis. In: Kliegman RM, St. Geme JW, Blum NJ, et al, eds. Nelson Textbook of Pediatrics. 22nd ed. Philadelphia, PA: Elsevier; 2025:chap 725.
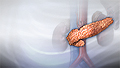
Osteomyelitis - illustration
Osteomyelitis is infection in the bones. Often, the original site of infection is elsewhere in the body, and spreads to the bone by the blood. Bacteria or fungus may sometimes be responsible for osteomyelitis.
Osteomyelitis
illustration

Review Date: 8/29/2024
Reviewed By: Jatin M. Vyas, MD, PhD, Professor in Medicine, Harvard Medical School; Associate in Medicine, Division of Infectious Disease, Department of Medicine, Massachusetts General Hospital, Boston, MA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.