Knee microfracture surgery
Cartilage regeneration - kneeKnee microfracture surgery is a common procedure used to repair damaged knee cartilage. Cartilage helps cushion and cover the area where bones meet in the joints.
Description
You will not feel any pain during the surgery. Three types of anesthesia may be used for knee arthroscopy surgery:
- Local anesthesia -- You will be given shots of painkillers to numb the knee. You may also be given medicines that relax you.
-
Spinal anesthesia -- The pain medicine is injected into a space in your spine. You will be awake, but will not be able to feel anything below your waist.
Spinal anesthesia
Spinal and epidural anesthesia are procedures that deliver medicines that numb parts of your body to block pain. They are given through shots in or ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Regional anesthesia -- The pain medicine is injected in your thigh and groin area. Your lower leg and knee will be numb after the injection.
-
General anesthesia -- You will be asleep and pain-free.
General anesthesia
General anesthesia is treatment with certain medicines that puts you into a deep sleep-like state so you do not feel pain during surgery. After you ...
Read Article Now Book Mark Article
The surgeon will perform the following steps:
- Make a one quarter-inch (6 mm) surgical cut on your knee.
- Place a long, thin tube with a camera on the end through this cut. This is called an arthroscope. The camera is attached to a video monitor in the operating room. This tool lets the surgeon look inside your knee area and work on the joint.
- Make another cut and pass tools through this opening. A small pointed tool called an awl is used to make very small holes in the bone near the damaged cartilage. This will cause a small amount of blood to come in contact with the defect. These are called microfractures.
These holes connect to the bone marrow to release cells that can build new cartilage to replace the damaged tissue.
Why the Procedure Is Performed
You may need this procedure if you have damage to the cartilage:
- In the knee joint
- Under the kneecap
The goal of this surgery is to prevent or slow further damage to the cartilage. This will help prevent knee arthritis. It can help you delay the need for a partial or total knee replacement.
This procedure is also used to treat knee pain due to cartilage injuries.
A surgery called matrix autologous chondrocyte implantation (MACI) or mosaicplasty can also be done for similar problems.
Risks
Risks of anesthesia and surgery in general are:
- Reactions to medicines
-
Breathing problems
Breathing problems
Breathing difficulty may involve:Difficult breathing Uncomfortable breathingFeeling like you are not getting enough air
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Bleeding
Bleeding
Bleeding is the loss of blood. Bleeding may be:Inside the body (internal)Outside the body (external)Bleeding may occur:Inside the body when blood le...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Blood clots
Blood clots
Blood clots are clumps that occur when blood hardens from a liquid to a solid. A blood clot that forms inside one of your veins or arteries is calle...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Infection
Risks of microfracture surgery are:
- Cartilage breakdown over time -- The new cartilage made by microfracture surgery is not as strong as the body's original cartilage. It can break down more easily.
- The area with the unstable cartilage can get bigger with time as the degeneration progresses. This can give you more symptoms and pain.
- Increased stiffness of the knee.
Before the Procedure
Always tell your health care provider and surgeon what medicines you are taking, including medicines, herbs, or supplements you bought without a prescription.
During the 2 weeks before your surgery:
-
Prepare your home.
Prepare your home
Before you go to the hospital for surgery, set up your home to make your recovery and life easier when you come back. Plan and do this well in advan...
Read Article Now Book Mark Article - You may need to stop taking medicines that make it harder for your blood to clot. These include aspirin, ibuprofen (Advil, Motrin), naproxen (Naprosyn, Aleve), and others.
- Ask your surgeon which medicines you should still take on the day of your surgery.
- If you have diabetes, heart disease, or other medical conditions, your surgeon will ask you to see the provider who treats you for these conditions before your surgery.
- Tell your surgeon if you have been drinking a lot of alcohol, more than 1 or 2 drinks a day.
-
If you smoke, try to stop. Ask your provider for help. Smoking can slow down wound and bone healing.
If you smoke, try to stop
Quitting smoking and other nicotine products, including e-cigarettes, before surgery can improve your recovery and outcome after surgery. Most people...
Read Article Now Book Mark Article - Always let your surgeon know about any cold, flu, fever, herpes breakout, or other illness you may have before your surgery.
On the day of your surgery:
- You may be asked not to drink or eat anything for 6 to 12 hours before the procedure.
- Take the medicines your surgeon told you to take with a small sip of water.
- Your surgeon or nurse will tell you when to arrive at the hospital.
After the Procedure
Physical therapy may begin in the recovery room right after your surgery. You will also need to use a machine, called a CPM machine. This machine will gently exercise your leg for 6 to 8 hours a day for several weeks. This machine is most often used for 6 weeks after surgery. Ask your surgeon how long you will use it.
After your surgery
You had arthroscopy to treat problems in your knee. This article discusses how to take care of yourself when you go home from the hospital.
Read Article Now Book Mark ArticleYour surgeon will increase the exercises you do over time until you can fully move your knee again. The exercises may make the new cartilage heal better.
You will need to keep your weight off your knee for 6 to 8 weeks unless told otherwise. You will need crutches to get around. Keeping the weight off the knee helps the new cartilage grow. Make sure you check with your surgeon to find out how much weight you can put on your leg and for how long.
Crutches
It is important to start walking as soon as you can after your surgery. But you will need support for walking while your leg heals. Crutches may be...
Read Article Now Book Mark ArticleYou will need to go to physical therapy and do exercises at home for 3 to 6 months after surgery.
Outlook (Prognosis)
Many people do well after this surgery. Recovery time can be slow. Many people can go back to sports or other intense activities in about 9 to 12 months. Athletes in very intense sports may not be able to return to their former level.
People under age 40 with a recent injury often have the best results. People who are not overweight also have better results.
References
Frank RM, Lehrman B, Yanke AB, Cole BJ. Chondroplasty and microfracture. In: Miller MD, Browne JA, Cole BJ, Cosgarea AJ, Owens BD, eds. Operative Techniques: Knee Surgery. 2nd ed. Philadelphia, PA: Elsevier; 2018:chap 10.
Frank RM, Vidal AF, McCarty EC. Frontiers in articular cartilage treatment. In: Miller MD, Thompson SR, eds. DeLee, Drez, & Miller's Orthopaedic Sports Medicine. 5th ed. Philadelphia, PA: Elsevier; 2020:chap 97.
Harris JD, Cole BJ. Knee articular cartilage restoration procedures. In: Noyes FR, Barber-Westin SD, eds. Noyes' Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes. 2nd ed. Philadelphia, PA: Elsevier; 2017:chap 31.
Miller RH, Azar FM. Knee injuries. In: Azar FM, Beaty JH, eds. Campbell's Operative Orthopaedics. 14th ed. Philadelphia, PA: Elsevier; 2021:chap 45.
-
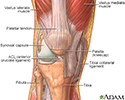
The structure of a joint - illustration
Joints, particularly hinge joints like the elbow and the knee, are complex structures made up of bone, muscles, synovium, cartilage, and ligaments that are designed to bear weight and move the body through space. The knee consists of the femur (thigh bone) above, and the tibia (shin bone) and fibula below. The kneecap (patella) glides through a shallow groove on the front part of the lower thigh bone. Ligaments and tendons connect the three bones of the knee, which are contained in the joint capsule (synovium) and are cushioned by cartilage.
The structure of a joint
illustration
-
The structure of a joint - illustration
Joints, particularly hinge joints like the elbow and the knee, are complex structures made up of bone, muscles, synovium, cartilage, and ligaments that are designed to bear weight and move the body through space. The knee consists of the femur (thigh bone) above, and the tibia (shin bone) and fibula below. The kneecap (patella) glides through a shallow groove on the front part of the lower thigh bone. Ligaments and tendons connect the three bones of the knee, which are contained in the joint capsule (synovium) and are cushioned by cartilage.
The structure of a joint
illustration
Review Date: 6/17/2024
Reviewed By: C. Benjamin Ma, MD, Professor, Chief, Sports Medicine and Shoulder Service, UCSF Department of Orthopaedic Surgery, San Francisco, CA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.