Tracheostomy
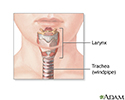
A tracheostomy is a surgical procedure to create an opening through the neck into the trachea (windpipe). A tube is most often placed through this opening to provide an airway and to remove secretions from the lungs. This tube is called a tracheostomy tube or trach tube.
Description
General anesthesia is used, unless the situation is critical. If that happens, a numbing medicine is placed into the area to help you feel less pain during the procedure. Other medicines are also given to relax and calm you (if there is time).
General anesthesia
General anesthesia is treatment with certain medicines that puts you into a deep sleep so you do not feel pain during surgery. After you receive the...
Read Article Now Book Mark ArticleThe neck is cleaned and draped. Surgical cuts are made to reveal the tough cartilage rings that form the outer wall of the trachea. The surgeon creates an opening into the trachea and inserts a tracheostomy tube.
Why the Procedure Is Performed
A tracheostomy may be done if you have:
- A large object blocking the airway
- An inability to breathe on your own
- An inherited abnormality of the larynx or trachea
- Breathed in harmful material such as smoke, steam, or other toxic gases that swell and block the airway
- Cancer of the neck, which can affect breathing by pressing on the airway
-
Paralysis of the muscles that affect swallowing
Paralysis
Muscle function loss is when a muscle does not work or move normally. The medical term for complete loss of muscle function is paralysis.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Severe neck or mouth injuries
- Surgery around the voice box (larynx) that prevents normal breathing and swallowing
Risks
The risks for any anesthesia are:
- Problems breathing
- Reactions to medicines, including heart attack and stroke, or allergic reaction (rash, swelling, breathing difficulty)
The risks for any surgery are:
- Bleeding
- Infection
- Nerve injury, including paralysis
- Scarring
Other risks include:
- Abnormal connection between the trachea and major blood vessels
- Damage to the thyroid gland
-
Erosion of the trachea (rare)
Erosion
Erosion is a breakdown of the outer layers of the skin, usually because of a: CutScrapeInflammation
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Puncture of the lung and lung collapse
- Scar tissue in the trachea that causes pain or trouble breathing
After the Procedure
A person may have a sense of panic and feel unable to breathe and speak when first waking up after the tracheostomy and placement of the tracheostomy tube. This feeling will lessen over time. Medicines may be given to help reduce the patient's stress.
If the tracheostomy is temporary (for example, if the condition leading to its placement can be improved), the tube will eventually be removed. Healing will occur quickly, leaving a small scar. Sometimes, a surgical procedure may be needed to close the site (stoma).
Occasionally a stricture, or tightening of the trachea may develop, which may affect breathing.
If the tracheostomy tube is permanent, the hole remains open.
Outlook (Prognosis)
Most people need 1 to 3 days to adapt to breathing through a tracheostomy tube. It will take some time to learn how to communicate with others. At first, it may be impossible for the person to talk or make sounds.
After training and practice, most people can learn to talk with a tracheostomy tube, many times by using special speaking valves. People or family members learn how to take care of the tracheostomy during the hospital stay. Home-care service may also be available.
You should be able to go back to your normal lifestyle. When you are outside, you can wear a loose covering (a scarf or other protection) over the tracheostomy stoma (hole). Use safety precautions when you are exposed to water, aerosols, powder, or food particles.
References
Cameron J. Chest wall, mediastinum, and trachea. In: Cameron J, ed. Current Surgical Therapy. 14th ed. Philadelphia, PA: Elsevier; 2023:chap 15.
Greenwood JC, Winters ME. Tracheostomy care. In: Roberts JR, Custalow CB, Thomsen TW, eds. Roberts and Hedges' Clinical Procedures in Emergency Medicine and Acute Care. 7th ed. Philadelphia, PA: Elsevier; 2019:chap 7.

 abnormality of the larynx or trachea; Severe neck or mouth injuries; Inhalation of corrosive material smoke or steam; Presence of a large foreign body that occludes the airway; Paralysis of the muscles that affect swallowing causing a danger of aspiration; Long term unconsciousness or coma.</p>")


 (a scarf or other protection) is recommended. Other safety precautions regarding exposure to water, aerosols, powder or food particles must be adhered to. After treatment of the underlying problem that necessitated the tracheostomy tube initially, the tube is easily removed, and the hole heals quickly, with only a small scar.</p>")
Review Date: 1/22/2023
Reviewed By: Denis Hadjiliadis, MD, MHS, Paul F. Harron, Jr. Professor of Medicine, Pulmonary, Allergy, and Critical Care, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.