

Ureteropelvic junction obstruction
Ureteropelvic junction obstruction; UP junction obstruction; Obstruction of the ureteropelvic junctionUreteropelvic junction (UPJ) obstruction is a blockage at the point where part of the kidney attaches to one of the tubes to the bladder (ureters). This blocks the flow of urine out of the kidney.
Causes
UPJ obstruction mostly occurs in children. It often happens when a baby is still growing in the womb. This is called a congenital condition (present from birth).
The blockage is caused when there is:
- A narrowing of area between the ureter and the part of the kidney called the renal pelvis
- An abnormal blood vessel crossing over the ureter
As a result, urine builds up and damages the kidney.
In older children and adults, the problem may be due to scar tissue, infection, earlier treatments for a blockage, or kidney stones.
UPJ obstruction is the most common cause of urinary blockages in children. It is now commonly found before birth with ultrasound tests. In some cases, the condition may not show up until after birth. Surgery may be needed early in life if the problem is severe. Most of the time, surgery is not needed until later. Some cases do not require surgery at all.
Symptoms
There may not be any symptoms. When symptoms occur, they may include:
- Back or flank pain especially when consuming diuretics such as alcohol or caffeine
Flank pain
Flank pain is pain in one side of the body between the upper belly area (abdomen) and the back.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Bloody urine (hematuria)
- Lump in the abdomen (abdominal mass)
- Kidney infection
- Poor growth in infants (failure to thrive)
- Urinary tract infection, usually with fever
Urinary tract infection
A urinary tract infection, or UTI, is an infection of the urinary tract. The infection can occur at different points in the urinary tract, including...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Vomiting
Exams and Tests
An ultrasound during pregnancy may show kidney problems in the unborn baby.
Tests after birth may include:
- BUN
BUN
BUN stands for blood urea nitrogen. Urea nitrogen is what forms when protein breaks down. A test can be done to measure the amount of urea nitrogen ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Creatinine clearance
Creatinine clearance
The creatinine clearance test helps provide information about how well the kidneys are working. The test compares the creatinine level in urine with...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - CT scan
- Electrolytes
Electrolytes
Electrolytes are minerals in your blood and other body fluids that carry an electric charge. Electrolytes affect how your body functions in many ways...
Read Article Now Book Mark Article - IVP -- less commonly used
IVP
An intravenous pyelogram (IVP) is a special x-ray exam of the kidneys, bladder, and ureters (the tubes that carry urine from the kidneys to the bladd...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - CT urogram -- scan of both kidneys and ureters with IV contrast
- Nuclear scan of kidneys
Nuclear scan of kidneys
A renal scan is a nuclear medicine exam in which a small amount of radioactive material (radioisotope) is used to measure the function of the kidneys...
ImageRead Article Now Book Mark Article - Voiding cystourethrogram
Voiding cystourethrogram
A voiding cystourethrogram is an x-ray study of the bladder and urethra. It is done while the bladder is emptying.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Ultrasound
Treatment
Surgery to correct the blockage allows urine to flow normally. Most of the time, open (invasive) surgery is performed in infants. Adults may be treated with less-invasive procedures. These procedures involve much smaller surgical cuts than open surgery, and may include:
- Endoscopic (retrograde) technique which does not require a surgical cut on the skin. Instead, a small instrument is placed into the urethra and bladder and into the affected ureter. This allows the surgeon to open the blockage from the inside.
- Percutaneous (antegrade) technique involves a small surgical cut on the side of the body between the ribs and the hip.
- Pyeloplasty removes scar tissue from the blocked area and reconnects the healthy part of the kidney to the healthy ureter.
Laparoscopy has also been used to treat UPJ obstruction in children and adults who have not had success with other procedures.
A tube called a stent may be placed to drain urine from the kidney until the surgery heals. A nephrostomy tube, which is placed in the side of the body to drain urine, may also be needed for a short time after the surgery. This type of tube may also be used to treat a bad infection before surgery.
Stent
A stent is a tiny tube placed into a hollow structure in your body. This structure can be an artery, a vein, or another structure, such as the tube ...

Outlook (Prognosis)
Detecting and treating the problem early can help prevent future kidney damage. UPJ obstruction diagnosed before birth or early after birth may actually improve on its own.
Most children do well and have no long-term problems. Serious damage may occur in people who are diagnosed later in life.
Long-term outcomes are good with current treatments. Pyeloplasty has the best long-term success.
Possible Complications
If untreated, UPJ obstruction can lead to permanent loss of kidney function (kidney failure).
Kidney failure
Acute kidney failure is the rapid (less than 2 days) loss of your kidneys' ability to remove waste and help balance fluids and electrolytes in your b...
Kidney stones or infection may occur in the affected kidney, even after treatment.
When to Contact a Medical Professional
Contact the health care provider if your infant has:
- Bloody urine
- Fever
- A lump in the abdomen
- Indications of back pain or pain in the flanks (the area toward the sides of the body between the ribs and the pelvis)
References
Chaudhry R, Cannon GM. Urologic disorders. In: Zitelli BJ, McIntire SC, Nowalk AJ, Garrison J, eds. Zitelli and Davis' Atlas of Pediatric Physical Diagnosis. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 15.
Elder JS. Obstruction of the urinary tract. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 555.
Frøkiaer J. Urinary tract obstruction. In: Yu ASL, Chertow GM, Luyckx VA, Marsden PA, Skorecki K, Taal MW, eds. Brenner and Rector's The Kidney. 11th ed. Philadelphia, PA: Elsevier; 2020:chap 37.
Nakada SY, Best SL. Management of upper urinary tract obstruction. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 89.
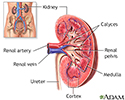
Kidney anatomy - illustration
The kidneys are responsible for removing wastes from the body, regulating electrolyte balance and blood pressure, and the stimulation of red blood cell production.
Kidney anatomy
illustration
Review Date: 4/1/2023
Reviewed By: Kelly L. Stratton, MD, FACS, Associate Professor, Department of Urology, University of Oklahoma Health Sciences Center, Oklahoma City, OK. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.