

Meniere disease
Hydrops; Hearing loss; Endolymphatic hydrops; Dizziness - Ménière disease; Vertigo - Ménière disease; Hearing loss - Ménière disease; Overpressure therapy - Ménière disease; Ménière disease; Ménière's diseaseMénière disease is an inner ear disorder that affects balance and hearing.
Causes
Your inner ear contains fluid-filled tubes called labyrinths. These tubes, along with a nerve in your skull, help you know the position of your body and help maintain your balance.
The exact cause of Ménière disease is unknown. It may occur when the pressure of the fluid in part of the inner ear gets too high.
In some cases, Ménière disease may be related to:
- Head injury
- Middle or inner ear infection
Ear infection
Suspected ear infections are one of the most common reasons parents take their children to their health care provider. The most common type of ear i...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Other risk factors include:
- Alcohol use
- Allergies
- Family history
- Recent cold or viral illness
- Smoking
-
Stress
Stress
Stress is a feeling of emotional or physical tension. It can come from any event or thought that makes you feel frustrated, angry, or nervous. Stres...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Use of certain medicines
Ménière disease is a fairly common disorder.
Symptoms
Attacks of Ménière disease often start without warning. They may occur daily or as rarely as once a year. The severity of each attack can vary. Some attacks may be severe and interfere with daily living activities.
Ménière disease usually has four main symptoms:
-
Hearing loss that varies over time
Hearing loss
Hearing loss is being partly or totally unable to hear sound in one or both ears.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Pressure in the ear
- Ringing or roaring in the affected ear, called tinnitus
Tinnitus
Tinnitus is the medical term for "hearing" noises in your ears. It occurs when there is no outside source of the sounds. Tinnitus is often called "r...
ImageRead Article Now Book Mark Article - Vertigo, or dizziness
Severe vertigo is the symptom that causes the most problems. With vertigo, you feel as though you are spinning or moving, or that the world is spinning around you.
- Nausea, vomiting, and sweating often occur.
- Symptoms get worse with sudden movement.
- Often, you will need to lie down and close your eyes.
- You may feel dizzy and off-balance for anywhere from 20 minutes to 24 hours.
Hearing loss is often only in one ear, but it may affect both ears.
- Hearing tends to improve between attacks, but gets worse over time.
- Low frequency hearing is lost first.
- You also may have roaring or ringing in the ear (tinnitus), along with a sense of pressure in your ear.
Other symptoms include:
- Headaches
- Pain or discomfort in the abdomen
- Nausea and vomiting
- Uncontrollable eye movements (a symptom called nystagmus)
Nystagmus
Nystagmus is a term to describe uncontrollable movements of the eyes that may be:Side to side (horizontal nystagmus)Up and down (vertical nystagmus)R...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Sometimes the nausea and vomiting are severe enough that you need to be admitted to the hospital to receive IV fluids or you need to rest at home.
Exams and Tests
A brain and nervous system exam may show problems with hearing, balance, or eye movement.
A hearing test will show the hearing loss that occurs with Ménière disease. Hearing may be near normal after an attack.
A caloric stimulation test checks your eye reflexes by warming and cooling the inner ear with water. Test results that are not in the normal range can be a sign of Ménière disease.
Caloric stimulation
Caloric stimulation is a test that uses differences in temperature to diagnose damage to the acoustic nerve. This is the nerve that is involved in h...

These tests may also be done to check for other causes of vertigo:
- Electrocochleography (ECOG)
-
Electronystagmography (ENG) or videonystagmography (VNG)
Electronystagmography
Electronystagmography is a test that looks at eye movements to see how well nerves in the brain are working. These nerves are:Vestibular nerve (eigh...
Read Article Now Book Mark Article -
Head MRI scan
Head MRI scan
A head MRI (magnetic resonance imaging) is an imaging test that uses powerful magnets and radio waves to create pictures of the brain and surrounding...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Treatment
There is no known cure for Ménière disease. However, lifestyle changes and some treatments can help relieve symptoms.
Your health care provider may suggest ways to reduce the amount of fluid in your body. This can often help control symptoms.
- Water pills (diuretics) may help relieve fluid pressure in the inner ear
- A low-salt diet may also help
Low-salt diet
Sodium is an element that the body needs to work properly. Salt contains sodium.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
To help ease symptoms and stay safe:
- Avoid sudden movements, which may worsen symptoms. You may need help walking during attacks.
- Avoid bright lights, TV, and reading during attacks. They can make symptoms worse.
- Do not drive, operate heavy machinery, or climb until 1 week after your symptoms disappear. A sudden dizzy spell during these activities can be dangerous.
- Remain still and rest when you have symptoms.
- Gradually increase your activity after attacks.
Symptoms of Ménière disease can cause stress. Make healthy lifestyle choices to help you cope:
- Eat a well-balanced, healthy diet. Don't overeat.
- Exercise regularly, if possible.
- Get enough sleep.
- Limit caffeine and alcohol.
Help ease stress by using relaxation techniques, such as:
- Guided imagery
- Meditation
- Progressive muscle relaxation
- Tai chi
- Yoga
Ask your provider about other self-care measures.
Self-care measures
You have seen your health care provider for Ménière disease. During Ménière attacks, you may have vertigo, or the feeling that you are spinning. Yo...
Read Article Now Book Mark ArticleYour provider may prescribe:
- Antinausea medicines to relieve nausea and vomiting
- Diazepam (Valium) or motion sickness medicines, such as meclizine (Antivert, Bonine, Dramamine) to relieve dizziness and vertigo
Other treatments that may be helpful include:
- A hearing aid to improve hearing in the affected ear.
- Balance therapy, which includes head, eye, and body exercises you can do at home to help train your brain to overcome dizziness.
- Overpressure therapy using a device that sends tiny pressure pulses through the ear canal to the middle ear. The pulses are aimed reducing amount of fluid in the middle ear, which in turn reduces dizziness.
You may need ear surgery if your symptoms are severe and do not respond to other treatments.
- Surgery to cut the vestibular nerve helps control vertigo. It does not damage hearing.
- Surgery to decompress a structure in the inner ear called the endolymphatic sac. Hearing may be affected by this procedure.
- Injecting steroids or an antibiotic called gentamicin directly into the middle ear can help control vertigo.
- Removing part of the inner ear (labyrinthectomy) helps treat vertigo. This causes complete hearing loss.
Support Groups
These resources can provide more information on Ménière disease:
- American Academy of Otolaryngology-Head and Neck Surgery -- www.enthealth.org/conditions/menieres-disease/
- National Institute on Deafness and Other Communication Disorders -- www.nidcd.nih.gov/health/menieres-disease
- Vestibular Disorders Association -- vestibular.org/menieres-disease
Outlook (Prognosis)
Ménière disease can often be controlled with treatment. Or, the condition may get better on its own. In some cases, Ménière disease can be chronic (long-term) or disabling.
When to Contact a Medical Professional
Call your provider if you have symptoms of Ménière disease, or if symptoms get worse. These include hearing loss, ringing in the ears, or dizziness.
Prevention
You can't prevent Ménière disease. Treating early symptoms right away may help prevent the condition from getting worse. Treating an ear infection and other related disorders may be helpful.
Ear infection
Otitis is a term for infection or inflammation of the ear.
References
Crane BT, Minor LB. Peripheral vestibular disorders. In: Flint PW, Haughey BH, Francis HW, et al, eds. Cummings Otolaryngology: Head and Neck Surgery. 7th ed. Philadelphia, PA: Elsevier; 2021:chap 167.
Holste K, Patil PG. Treatment of intractable vertigo. In: Winn HR, ed. Youmans and Winn Neurological Surgery. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 128.
National Institute on Deafness and Other Communicable Diseases website. Meniere's disease. www.nidcd.nih.gov/health/menieres-disease. Updated February 13, 2017. Accessed September 8, 2023.
-
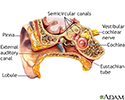
Ear anatomy - illustration
The ear consists of external, middle, and inner structures. The eardrum and the 3 tiny bones conduct sound from the eardrum to the cochlea.
Ear anatomy
illustration
-
Tympanic membrane - illustration
The tympanic membrane is also called the eardrum. It separates the outer ear from the middle ear. When sound waves reach the tympanic membrane they cause it to vibrate. The vibrations are then transferred to the tiny bones in the middle ear. The middle ear bones then transfer the vibrating signals to the inner ear. The tympanic membrane is made up of a thin connective tissue membrane covered by skin on the outside and mucosa on the internal surface.
Tympanic membrane
illustration

-
Ear anatomy - illustration
The ear consists of external, middle, and inner structures. The eardrum and the 3 tiny bones conduct sound from the eardrum to the cochlea.
Ear anatomy
illustration
-
Tympanic membrane - illustration
The tympanic membrane is also called the eardrum. It separates the outer ear from the middle ear. When sound waves reach the tympanic membrane they cause it to vibrate. The vibrations are then transferred to the tiny bones in the middle ear. The middle ear bones then transfer the vibrating signals to the inner ear. The tympanic membrane is made up of a thin connective tissue membrane covered by skin on the outside and mucosa on the internal surface.
Tympanic membrane
illustration
Review Date: 8/28/2023
Reviewed By: Joseph V. Campellone, MD, Department of Neurology, Cooper Medical School at Rowan University, Camden, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.