
Cystitis - acute
Uncomplicated urinary tract infection; UTI - acute cystitis; Acute bladder infection; Acute bacterial cystitisAcute cystitis is an infection of the bladder or lower urinary tract. Acute means that the infection begins suddenly.
Causes
Cystitis is caused by germs, most often bacteria. These germs enter the urethra and then the bladder and can cause an infection. The infection commonly develops in the bladder. It can also spread to the kidneys.
Most of the time, your body can get rid of these bacteria when you urinate. But, the bacteria can stick to the wall of the urethra or bladder, or grow so fast that some stay in the bladder.
Women tend to get infections more often than men. This happens because their urethra is shorter and closer to the anus. Women are more likely to get an infection after sexual intercourse. Using a diaphragm for birth control can also be a cause. Menopause also increases the risk for a urinary tract infection.
Menopause
Menopause is the time in a woman's life when her periods (menstruation) stop. Most often, it is a natural, normal body change that occurs between ag...

The following also increase your chances of having cystitis:
- A tube called a urinary catheter inserted in your bladder
Urinary catheter
A urinary catheter is a tube placed in the body to drain and collect urine from the bladder.
Read Article Now Book Mark Article - Blockage of the bladder or urethra
-
Diabetes
Diabetes
Diabetes is a long-term (chronic) disease in which the body cannot regulate the amount of sugar in the blood.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Enlarged prostate, narrowed urethra, or anything that blocks the flow of urine
Enlarged prostate
The prostate is a gland that produces some of the fluid that carries sperm during ejaculation. The prostate gland surrounds the urethra, the tube th...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleNarrowed urethra
Urethral stricture is an abnormal narrowing of the urethra. The urethra is the tube that carries urine out of the body from the bladder.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Loss of bowel control (bowel incontinence)
Bowel incontinence
Bowel incontinence is the loss of bowel control, causing you to unexpectedly pass stool. This can range from sometimes leaking a small amount of sto...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Older age (most often in people who live in nursing homes)
- Pregnancy
- Problems fully emptying your bladder (urinary retention)
- Procedures that involve the urinary tract
- Staying still (immobile) for a long period of time (for example, when you are recovering from a hip fracture)
Hip fracture
If more pressure is put on a bone than it can stand, it will split or break. A break of any size is called a fracture. If the broken bone punctures...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Most cases are caused by Escherichia coli (E coli). It is a type of bacteria found in the intestines.
Symptoms
The symptoms of a bladder infection include:
- Cloudy or bloody urine
- Strong or foul-smelling urine
- Low fever (most people will not have a fever)
- Pain or burning with urination
- Pressure or cramping in the lower middle abdomen or back
- Strong need to urinate often, even right after the bladder has been emptied
Often in an older person, mental changes or confusion are the only signs of a possible infection.
Exams and Tests
In most cases, a urine sample is collected to do the following tests:
-
Urinalysis -- This test is done to look for white blood cells, red blood cells, bacteria, and to check for certain chemicals, such as nitrites in the urine. Most of the time, your health care provider can diagnose an infection using a urinalysis.
Urinalysis
Urinalysis is the physical, chemical, and microscopic examination of urine. It involves a number of tests to detect and measure various compounds th...
ImageRead Article Now Book Mark Article - Urine culture -- A clean catch urine sample may be needed. This test is done to identify the bacteria in the urine and decide on the correct antibiotic. This is often not needed to start treatment of cystitis.
A clean catch urine sample
A urine culture is a lab test to check for bacteria or other germs in a urine sample. It can be used to check for a urinary tract infection in adults...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Treatment
Antibiotics can be taken by mouth. These are most often given to stop the infection from spreading to the kidneys.
For a simple bladder infection, you will take antibiotics for 3 days (women) or 7 to 14 days (men). For a bladder infection with complications such as pregnancy, diabetes, or a mild kidney infection, you will most often take antibiotics for 7 to 14 days.
Diabetes
Diabetes is a long-term (chronic) disease in which the body cannot regulate the amount of sugar in the blood.
It is important that you finish all the antibiotics prescribed. Finish them even if you feel better before the end of your treatment. If you do not finish the antibiotics, you may develop an infection that is harder to treat.
Let your provider know if you are pregnant.
Your provider may prescribe medicines to ease discomfort. Phenazopyridine hydrochloride (Pyridium) is the most common of this type of drug. You will still need to take antibiotics.
Everyone with a bladder infection should drink plenty of water.
Some women have repeat bladder infections. Your provider may suggest treatments such as:
- Taking a single dose of an antibiotic after sexual contact. These may prevent sexually transmitted infections.
- Keeping a 3-day course of antibiotics. These will be given based on your symptoms.
- Taking a single, daily dose of an antibiotic. This dose will prevent infections.
Over-the-counter products that increase acid in the urine, such as ascorbic acid or cranberry juice, may be recommended. These medicines lower the concentration of bacteria in the urine.
Ascorbic acid
Vitamin C is a water-soluble vitamin. It is needed for normal growth and development. Water-soluble vitamins dissolve in water. Leftover amounts of...

Follow-up may include urine cultures. These tests will make sure the bacterial infection is gone.
Lifestyle changes may help prevent some urinary tract infections.
Lifestyle changes
Most urinary tract infections (UTIs) are caused by bacteria that enter the urethra and travel to the bladder.
Outlook (Prognosis)
Most cases of cystitis are uncomfortable, but go away without complications after treatment.
When to Contact a Medical Professional
Contact your provider if you:
- Have symptoms of cystitis
- Have already been diagnosed and symptoms get worse
- Develop new symptoms such as fever, back pain, stomach pain, or vomiting
Fever
Fever is the temporary increase in the body's temperature in response to a disease or illness. A child has a fever when the temperature is at or abov...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleVomiting
Nausea is feeling an urge to vomit. It is often called "being sick to your stomach. "Vomiting or throwing-up forces the contents of the stomach up t...
ImageRead Article Now Book Mark Article
References
Cooper KL, Badalato GM, Rutman MP. Infections of the urinary tract. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh-Wein Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 55.
Nicolle LE, Drekonja D. Approach to the patient with urinary tract infection. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier; 2020:chap 268.
Sobel JD, Brown P. Urinary tract infections. In: Bennett JE, Dolin R, Blaser MJ, eds. Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases. 9th ed. Philadelphia, PA: Elsevier; 2020:chap 72.
-
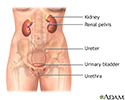
Female urinary tract - illustration
The female and male urinary tracts are relatively the same except for the length of the urethra.
Female urinary tract
illustration
-
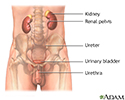
Male urinary tract - illustration
The male and female urinary tracts are relatively the same except for the length of the urethra.
Male urinary tract
illustration
-
Female urinary tract - illustration
The female and male urinary tracts are relatively the same except for the length of the urethra.
Female urinary tract
illustration
-
Male urinary tract - illustration
The male and female urinary tracts are relatively the same except for the length of the urethra.
Male urinary tract
illustration
Review Date: 8/15/2022
Reviewed By: Linda J. Vorvick, MD, Clinical Professor, Department of Family Medicine, UW Medicine, School of Medicine, University of Washington, Seattle, WA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.