
Alport syndrome
Hereditary nephritis; Hematuria - nephropathy - deafness; Hemorrhagic familial nephritis; Hereditary deafness and nephropathyAlport syndrome is a rare inherited disorder that damages the tiny blood vessels in the kidneys. It can also cause hearing loss and eye problems.
Causes
Alport syndrome is an inherited form of kidney inflammation (nephritis). It is caused by a defect (mutation) in a gene for a protein in the connective tissue, called collagen.
The disorder is rare. There are three genetic types:
- X-linked Alport syndrome (XLAS) -- This is the most common type. The disease is more severe in males than in females.
- Autosomal recessive Alport syndrome (ARAS) -- Males and females have equally severe disease.
- Autosomal dominant Alport syndrome (ADAS) -- This is the rarest type. Males and females have equally severe disease.
With all types of Alport syndrome, the kidneys are affected. The tiny blood vessels in the glomeruli of the kidneys are damaged. The glomeruli filter blood to make urine and remove waste products from the blood.
At first, there are no symptoms. Over time, as the glomeruli are more and more damaged, kidney function is lost and waste products and fluids build up in the body. The condition can progress to end-stage renal disease (ESRD) at an early age, between adolescence and age 40. At this point, dialysis or a kidney transplant is needed.
ESRD
End-stage kidney disease (ESKD) is the last stage of long-term (chronic) kidney disease. This is when your kidneys can no longer support your body's...

Dialysis
Dialysis treats end-stage kidney failure. It removes waste from your blood when your kidneys can no longer do their job. There are different types o...
Kidney transplant
A kidney transplant is surgery to place a healthy kidney into a person with kidney failure.
Symptoms
The main symptom of Alport syndrome is blood in the urine that is often not visible and only detected under a microscope. This occurs from a young age. As the disease progresses, other symptoms may appear.
KIDNEYS
Other symptoms of kidney problems include:
-
Abnormal urine color
Abnormal urine color
The usual color of urine is straw-yellow. Abnormally-colored urine may be cloudy, dark, or blood-colored.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Blood in the urine that is visible during a cold or flu or exercise
- Flank pain
- High blood pressure
-
Swelling throughout the body (edema)
Swelling throughout the body
Swelling is the enlargement of organs, skin, or other body parts. It is caused by a buildup of fluid in the tissues. The extra fluid can lead to a ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Fatigue
- Poor appetite
- Excessive thirst
EARS
Over time, Alport syndrome also leads to hearing loss in both ears. By the early teens, it is common in males with XLAS, though in females, hearing loss is not as common and happens when they're adults. With ARAS, boys and girls have hearing loss during childhood. With ADAS, it occurs later in life.
Hearing loss usually occurs before kidney failure.
EYES
Alport syndrome also leads to eye problems in those with XLAS and ARAS, including:
- Abnormal shape of the lens (anterior lenticonus), which can lead to a slow decline in vision as well as cataracts.
- Corneal erosion in which there is damage to the outer layer of the covering of the eyeball, leading to pain, itching, redness of the eye, or blurred vision.
- Abnormal coloring of the retina, a condition called dot-and-fleck retinopathy. It doesn't cause vision problems, but can help diagnose Alport syndrome.
Retina
The retina is the light-sensitive layer of tissue at the back of the eyeball. Images that come through the eye's lens are focused on the retina. Th...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Macular hole in which there is thinning or a break in the macula. The macula is a part of the retina that makes central vision sharper and more detailed. A macular hole causes blurred or distorted central vision.
Eye problems are uncommon in people with ADAS.
Exams and Tests
The health care provider will examine you and ask about your symptoms.
The following tests may be done:
-
BUN and serum creatinine
BUN
BUN stands for blood urea nitrogen. Urea nitrogen is what forms when protein breaks down. A test can be done to measure the amount of urea nitrogen ...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleCreatinine
The creatinine blood test measures the level of creatinine in the blood. This test is done to see how well your kidneys are working. Creatinine in t...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Complete blood count
Complete blood count
A complete blood count (CBC) test measures the following:The number of white blood cells (WBC count)The number of red blood cells (RBC count)The numb...
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article -
Renal biopsy
Renal biopsy
A kidney biopsy is the removal of a small piece of kidney tissue for examination.
ImageRead Article Now Book Mark Article -
Urinalysis
Urinalysis
Urinalysis is the physical, chemical, and microscopic examination of urine. It involves a number of tests to detect and measure various compounds th...
ImageRead Article Now Book Mark Article
If your provider suspects you have Alport syndrome, you will also likely have vision and hearing tests.
Treatment
The goals of treatment include monitoring and controlling the disease and treating the symptoms.
Your provider may recommend any of the following:
- A diet that limits salt, fluids, and potassium
- Medicines to control high blood pressure
Kidney disease is managed by:
- Taking medicines to slow kidney damage
- A diet that limits salt, fluids, and protein
Hearing loss can be managed with hearing aids. Eye problems are treated as needed. For example, an abnormal lens due to lenticonus or cataracts can be replaced.
Genetic counseling may be recommended because the disorder is inherited.
Support Groups
More information and support for people with Alport syndrome and their families can be found at:
- Alport Syndrome Foundation -- alportsyndrome.org/for-patients/patient-resources/
- National Kidney Foundation -- www.kidney.org/atoz/content/alport
- National Organization for Rare Disorders -- rarediseases.org/rare-diseases/alport-syndrome
Outlook (Prognosis)
The outlook depends on the type of Alport syndrome, biological sex, and age.
For both males and females, kidney function will worsen over time. In males with XLAS, this may lead to kidney failure at an earlier age. Most men with XLAS will experience kidney failure by age 60. Women with XLAS may or may not have kidney problems, but the risk increases with age.
Both males and females with ARAS will develop kidney failure by early adulthood.
ADAS progresses slowly in both males and females, and kidney failure may not occur until later in life.
As kidneys fail, dialysis or a kidney transplant will be needed. Kidney transplant is often very successful in people with Alport syndrome.
When to Contact a Medical Professional
Contact your provider for an appointment if:
- You have symptoms of Alport syndrome.
- You have a family history of Alport syndrome and you are planning to get pregnant.
- Your urine output decreases or stops or you see blood in your urine (this may be a symptom of chronic kidney disease).
Prevention
Awareness of risk factors, such as a family history of the disorder, may allow the condition to be detected early.
References
Gregory MC. Alport syndrome and related disorders. In: Gilbert SJ, Weiner DE, Bomback AS, Perazella MA, Rifkin DE, eds. National Kidney Foundation's Primer on Kidney Diseases. 8th ed. Philadelphia, PA: Elsevier; 2023:chap 41.
Radhakrishnan J, Appel GB, D'Agati VD. Secondary glomerular disease. In: Yu ASL, Chertow GM, Luyckx VA, Marsden PA, Skorecki K, Taal MW, eds. Brenner and Rector's The Kidney. 11th ed. Philadelphia, PA: Elsevier; 2020:chap 32.
Rheault MN, Kashtan CE. Alport syndrome and other familial glomerular syndromes. In: Johnson RJ, Floege J, Tonelli M, eds. Comprehensive Clinical Nephrology. 7th ed. Philadelphia, PA: Elsevier; 2024:chap 48.
-
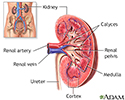
Kidney anatomy - illustration
The kidneys are responsible for removing wastes from the body, regulating electrolyte balance and blood pressure, and the stimulation of red blood cell production.
Kidney anatomy
illustration
Review Date: 5/19/2023
Reviewed By: Walead Latif, MD, Nephrologist and Clinical Associate Professor, Rutgers Medical School, Newark, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.