
Solitary pulmonary nodule
Lung cancer - solitary nodule; Infectious granuloma - pulmonary nodule; SPNA solitary pulmonary nodule is a round or oval spot (lesion) in the lung that is seen with a chest x-ray or CT scan.
Chest x-ray
A chest x-ray is an x-ray of the chest, lungs, heart, large arteries, ribs, and diaphragm.

CT scan
A chest CT (computed tomography) scan is an imaging method that uses x-rays to create cross-sectional pictures of the chest and upper abdomen....

Causes
More than half of all solitary pulmonary nodules are noncancerous (benign). Benign nodules have many causes, including scars and past infections.
Infectious granulomas (which are formed by cells as a reaction to a past infection) cause most benign nodules. Common infections that often result in granulomas or other healed scars include:
-
Tuberculosis (TB) or exposure to TB
Tuberculosis
Pulmonary tuberculosis (TB) is a contagious bacterial infection that involves the lungs. It may spread to other organs.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article - Fungus, such as aspergillosis, coccidioidomycosis, cryptococcosis, or histoplasmosis
Aspergillosis
Aspergillosis is an infection or allergic response due to the aspergillus fungus.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleCoccidioidomycosis
Valley fever is an infection that occurs when the spores of the fungus Coccidioides immitis enter your body through the lungs.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleCryptococcosis
Cryptococcosis is infection with the fungi Cryptococcus neoformans or Cryptococcus gattii.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark ArticleHistoplasmosis
Histoplasmosis is an infection that occurs from breathing in the spores of the fungus Histoplasma capsulatum.
 ImageRead Article Now Book Mark Article
ImageRead Article Now Book Mark Article
Primary lung cancer is the most common cause of cancerous (malignant) pulmonary nodules. This is cancer that starts in the lung.
Symptoms
A solitary pulmonary nodule itself rarely causes symptoms.
Exams and Tests
A solitary pulmonary nodule is most often found on a chest x-ray or chest CT scan. These imaging tests are often done for other symptoms or reasons. It can also occur as part of the screening chest CT for people age 50 to 80 years who have a 20 pack-year smoking history.
Your health care provider must decide whether the nodule in your lung is most likely benign or of concern. A nodule more is likely benign if:
- The nodule is small, has a smooth border, and has a solid and even appearance on an x-ray or CT scan.
- You are young and never smoked.
Your provider may then choose to monitor the nodule over time by repeating a series of x-rays or CT scans.
- Repeat chest x-rays or chest CT scans are the most common way to monitor the nodule. Sometimes, lung PET scans may be done.
PET scans
A lung positron emission tomography (PET) scan is an imaging test. It uses a radioactive substance (called a tracer) to look for disease in the lung...
Read Article Now Book Mark Article - If repeated x-rays show that the nodule size has not changed in 2 years, it is most likely benign and a biopsy is not needed.
Your provider may recommend a biopsy of the nodule to check for cancer if:
- You are a smoker.
- You have other symptoms of lung cancer.
- The nodule has grown in size or has changed when compared to earlier images.
- The nodule has features that make it more likely to be cancerous (malignant).
A lung needle biopsy may be done by placing a needle directly through the wall of your chest, or during procedures called bronchoscopy or mediastinoscopy.
Lung needle biopsy
A lung needle biopsy is a method to remove a piece of lung tissue for examination. If it is done through the wall of your chest, it is called a tran...

Bronchoscopy
Bronchoscopy is a test to view the airways and diagnose lung disease. It may also be used during the treatment of some lung conditions.

Mediastinoscopy
Mediastinoscopy with biopsy is a procedure in which a lighted instrument (mediastinoscope) is inserted in the space in the chest between the lungs (m...

Tests to check for TB and other infections may also be done.
Treatment
Ask your provider about the risks of having a biopsy versus monitoring the size of the nodule with regular x-rays or CT scans. Treatment may be based on the results of the biopsy or other tests.
Outlook (Prognosis)
The outlook is usually good if the nodule is benign. If the nodule does not grow larger over a 2-year period, often nothing more needs to be done.
References
Bueno J, Landeras L, Chung JH. Updated Fleischner Society guidelines for managing incidental pulmonary nodules: common questions and challenging scenarios. Radiographics. 2018;38(5):1337-1350. PMID: 30207935 pubmed.ncbi.nlm.nih.gov/30207935/.
Jokerst CE, Gotway MB. Thoracic radiology: noninvasive diagnostic imaging. In: Broaddus VC, Ernst JD, King TE, et al, eds. Murray and Nadel's Textbook of Respiratory Medicine. 7th ed. Philadelphia, PA: Elsevier; 2022:chap 20.
Reed JC. Solitary pulmonary nodule. In: Reed JC, ed. Chest Radiology: Patterns and Differential Diagnoses. 7th ed. Philadelphia, PA: Elsevier; 2018:chap 20.
-
Adenocarcinoma - chest x-ray - illustration
This chest x-ray shows adenocarcinoma of the lung. There is a rounded light spot in the right upper lung (left side of the picture) at the level of the second rib. The light spot has irregular and poorly defined borders and is not uniform in density. Diseases that may cause this type of x-ray result would be tuberculous or fungal granuloma, and malignant or benign tumors.
Adenocarcinoma - chest x-ray
illustration
-
Pulmonary nodule - front view chest x-ray - illustration
This x-ray shows a single lesion (pulmonary nodule) in the upper right lung (seen as a light area on the left side of the picture). The nodule has distinct borders (well-defined) and is uniform in density. Tuberculosis (TB) and other diseases can cause this type of lesion.
Pulmonary nodule - front view chest x-ray
illustration
-
Pulmonary nodule, solitary - CT scan - illustration
This CT scan shows a single lesion (pulmonary nodule) in the right lung. This nodule is seen as the light circle in the upper portion of the dark area on the left side of the picture. A normal lung would look completely black in a CT scan.
Pulmonary nodule, solitary - CT scan
illustration
-
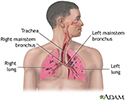
Respiratory system - illustration
Air is breathed in through the nasal passageways, travels through the trachea and bronchi to the lungs.
Respiratory system
illustration



-
Adenocarcinoma - chest x-ray - illustration
This chest x-ray shows adenocarcinoma of the lung. There is a rounded light spot in the right upper lung (left side of the picture) at the level of the second rib. The light spot has irregular and poorly defined borders and is not uniform in density. Diseases that may cause this type of x-ray result would be tuberculous or fungal granuloma, and malignant or benign tumors.
Adenocarcinoma - chest x-ray
illustration
-
Pulmonary nodule - front view chest x-ray - illustration
This x-ray shows a single lesion (pulmonary nodule) in the upper right lung (seen as a light area on the left side of the picture). The nodule has distinct borders (well-defined) and is uniform in density. Tuberculosis (TB) and other diseases can cause this type of lesion.
Pulmonary nodule - front view chest x-ray
illustration
-
Pulmonary nodule, solitary - CT scan - illustration
This CT scan shows a single lesion (pulmonary nodule) in the right lung. This nodule is seen as the light circle in the upper portion of the dark area on the left side of the picture. A normal lung would look completely black in a CT scan.
Pulmonary nodule, solitary - CT scan
illustration
-
Respiratory system - illustration
Air is breathed in through the nasal passageways, travels through the trachea and bronchi to the lungs.
Respiratory system
illustration
Review Date: 8/13/2023
Reviewed By: Denis Hadjiliadis, MD, MHS, Paul F. Harron Jr. Professor of Medicine, Pulmonary, Allergy, and Critical Care, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.