

Narcolepsy - InDepth
Daytime sleep disorder - InDepth; Cataplexy - InDepthAn in-depth report on the causes, diagnosis, and treatment of narcolepsy.
Highlights
Overview
Narcolepsy is a chronic neurological disorder. There are two types of narcolepsy, type 1 and type 2.
The defining characteristic of narcolepsy is excessive daytime sleepiness (EDS). EDS is perceived as periods of feeling an irrepressible need for sleep or being unable to stay awake during the day. Lapsing into sleep occurs unintentionally, several times in the same day and several days a week.
Besides EDS, people with narcolepsy type 1 also have cataplexy, which is a sudden but temporary muscle weakness, sometimes brought on by laughter or other emotions. Narcolepsy type 2 is defined as narcolepsy without cataplexy.
Narcolepsy affects about 26 to 79 out of 100,000 people. It is estimated that around half of people with narcolepsy in the US are not diagnosed or misdiagnosed.
Genetic Basis
Having a family member with narcolepsy presents a 20 to 40 times higher risk of developing the condition compared to the general population. Around 90% of patients with narcolepsy type 1 (narcolepsy with cataplexy) and half of patients with narcolepsy type 2 (narcolepsy without cataplexy) carry a specific genetic variation, called a haplotype, in an immune system gene (HLA-DQB1*06:02).
Causes
- Type 1 narcolepsy (narcolepsy with cataplexy), the most common form of the condition, is caused by a deficiency in the neurotransmitter hypocretin (orexin).
- The deficiency is thought to be a complex autoimmune process where the neurons that produce this protein are attacked by the immune system.
- Genetically, most patients with type 1 narcolepsy and many patients with type 2 narcolepsy carry HLA-DQB1*06:02.
- Upper airway infections from strep or influenza may trigger narcolepsy.
- The cause of narcolepsy type 2 (without cataplexy) is still unknown. Hypocretin levels are normal in this form of narcolepsy.
- Narcolepsy is not caused by mental illness or psychological problems, though it is often mistaken for such.
Diagnosis
Clinical features of narcolepsy invariably include EDS. The presence of cataplexy supports a diagnosis of type-I narcolepsy. Other clinical features can be present in, and supportive of type-I or type-II narcolepsy, including hypnagogic hallucinations and sleep paralysis.
Diagnosis can be confirmed by measuring spinal fluid hypocretin levels and performing sleep studies.
- Timely diagnosis can be a challenge. The condition is often overlooked or misdiagnosed.
- Narcolepsy is often hard to detect because sleep habits are not something typically asked about in a wellness visit.
Treatment
Treatment for narcolepsy is focused on controlling symptoms such as EDS and cataplexy and includes:
- Modafinil (Provigil) and armodafinil (Nuvigil) for excessive daytime sleepiness (EDS).
- Sodium oxybate (Xyrem, generic) for cataplexy as well as for EDS.
- When these drugs do not work, amphetamine-like stimulants or certain antidepressants may be used.
Introduction
Narcolepsy is considered a primary hypersomnia (excessive sleepiness) condition. Primary means the condition is not caused by another disease. The word narcolepsy comes from two Greek words roughly translated as "seized by numbness." The two primary symptoms in narcolepsy reflect this phrase:
- Excessive daytime sleepiness, with frequent daily sleep attacks or a need to take several naps during the day.
- Temporary and sudden muscle weakness without loss of consciousness (called cataplexy), usually brought on by sudden or strong emotions.
Some people experience other symptoms:
- Microsleep episodes, in which the patient behaves automatically but without conscious awareness.
- Sleep paralysis, a temporary inability to move or speak that occurs in the periods between wakefulness and sleep.
- Vivid dreamlike states between waking and sleeping (called hypnagogic or hypnopompic hallucinations).
Rapid eye movement (REM) sleep is abnormal in narcolepsy. REM sleep is the active, dreaming phase of sleep. In fact, narcolepsy is sometimes defined as the loss of boundaries between wakefulness, non-REM sleep, and REM sleep.
Primary Symptoms of Narcolepsy
Excessive Daytime Sleepiness
All people with narcolepsy can experience excessive sleepiness during the day. Sometimes they fall asleep rapidly and inappropriately, even when fully involved in an activity. This symptom is sometimes described as an irresistible daytime need for naps, which will generally refresh the person. EDS may be characterized by the following behaviors:
- People typically have periods of drowsiness every 3 or 4 hours that usually end in short naps.
- People may sleep during the day for a few minutes, particularly if they are in an awkward position for sleep or for a few hours if they are lying down.
- People often underestimate the duration of their drowsy periods and may not recall clearly their behavior during that time.
Cataplexy
Cataplexy is a brief and sudden loss of muscle tone or strength that results in an inability to move and always occurs during wakefulness. Symptoms of excessive daytime sleepiness may be present for years before cataplexy first occurs, although cataplexy often develops within a year. About two-thirds of people with narcolepsy have symptoms of cataplexy, and cataplexy is rarely present outside narcolepsy. The following events may be triggers for cataplexy:
- Sudden emotions, usually laughter (the most common trigger) and sometimes excitement, rage, or anger
- Surprise
- Sexual arousal
Muscle tone is completely absent during a cataplectic attack. Cataplectic attacks can be very minimal and appear as passing weakness, jaw-opening grimaces, or affecting only the eyelids and face. They may, on the other hand, be so severe that they weaken the whole body. In the most severe form of cataplexy, attacks can recur repeatedly for hours or days. This severe form of cataplexy is most often seen in children with narcolepsy, but can also occur from abrupt withdrawal from certain drugs used to treat narcolepsy, notably clomipramine.
Cataplexy may have the following characteristics:
- Most attacks last 30 seconds to 2 minutes and can be missed by even skilled observers. However, in severe cases, a person may fall and remain paralyzed for as long as several minutes.
- Typically the person's head suddenly falls forward, the jaw becomes slack, the arms drop to the side, and the knees buckle.
- Speech may become suddenly loud or broken and stutter-like.
Other Symptoms of Narcolepsy
Sleep paralysis
Sleep paralysis or atonia is a sense of paralysis that occurs in the periods between wakefulness and sleep. The person is conscious but cannot speak, move (cannot even open their eyes), or breathe deeply. Sleep paralysis rarely lasts beyond 20 minutes, but when it first occurs the experience can be terrifying, particularly if the patient also develops hallucinations.
Hypnagogic Hallucinations
Hypnagogic hallucinations are dreams that intrude on wakefulness, which can cause visual, auditory, or touching sensations. They occur between waking and sleeping, usually at the onset of sleep, and can also occur about 30 seconds after a cataplectic attack. Similar symptoms may occur while falling asleep (hypnopompic hallucinations).
- Visual hallucinations have been described as a "film running through the head" or as a waking dream with strong emotional content. Images can be intrusive. More commonly they may involve seeing colored forms that shift in size and shape.
- Auditory hallucinations may include random sounds or elaborate melodies.
- A person may also hallucinate feelings of rubbing or light touches, even levitation.
Such symptoms may also appear in other sleep disorders and are probably related to extreme sleepiness. In general, cataplexy must also be present for a clear diagnosis of narcolepsy. It is possible, however, for some people with narcolepsy to experience hypnagogic or hypnopompic hallucinations and daytime sleepiness and not cataplexy.
Microsleep and Automatic Behavior
In some cases, people have so-called microsleep episodes, in which they behave automatically without conscious awareness. Such automatic behavior may not be recognized as part of a disorder by either patients or the people around them. Some examples include:
- People with narcolepsy can be driving or walking competently but end up in a location different from the intended one.
- A person with narcolepsy can be carrying on a conversation and jump from one unrelated topic to another or just trail off and stop talking altogether.
- The person may suddenly perform bizarre actions, such as putting socks in the refrigerator.
- People may have severe forgetfulness.
- Their movements may suddenly become slow or clumsy.
- In some cases, their behavior may resemble some forms of epileptic seizures.
Disturbed Sleep
People with narcolepsy often have trouble staying asleep due to various disturbances. The disturbances, such as insomnia, vivid dreams, sleep talking, acting out while dreaming, or periodic limb movement disorder, are usually mild to moderate and do not account for the daytime sleepiness experienced by people with narcolepsy.
Periodic Limb Movement Disorder
Many people with narcolepsy experience periodic limb movement disorder (PLMD, formerly known as nocturnal myoclonus). In PLMD, the leg muscles involuntarily contract every 20 to 40 seconds during sleep, occasionally arousing the person. The person is usually unaware of the limb movements, but bed partners may notice the movements.
Healthy Sleep
Most people need about 8 hours of sleep each day, however individual adults differ in the amount of sleep they need to feel well-rested. Infants may sleep as many as 16 hours a day.
The daily cycle of life, which includes sleeping and waking, is called a circadian (meaning "about a day") rhythm, commonly referred to as the biological clock. Hundreds of bodily functions follow biologic clocks, but sleeping and waking comprise the most prominent circadian rhythm. The sleeping and waking cycle is about 24 hours. If confined to windowless apartments, with no clocks or other time cues, and sleeping and waking as their bodies dictate, humans typically live on slightly longer than 24-hour cycles. The daily sleep/wake cycle usually follows the following pattern:
- Humans function best with daytime activity and nighttime rest.
- Additionally, there is a natural peak in sleepiness at mid-day, the traditional siesta time.
Daily rhythms intermesh with other factors that may interfere or change individual patterns:
- The fraction-of-a-second-firing of nerve cells in the brain may be faster or slower in different individuals.
- The monthly menstrual cycle in women can shift the pattern.
- Light signals coming through the eyes reset the circadian cycles each day, so changes in season or various exposures to light and dark can unsettle the pattern. Sunlight is an important cue for circadian rhythms and is shown by the problems experienced by people who are blind. They commonly have trouble sleeping and experience other biorhythm disruptions.
Sleep Cycles
Sleep consists of two distinct states that alternate in cycles and reflect differing levels of brain nerve cell activity.
Non-Rapid Eye Movement Sleep (Non-REM)
Non-REM sleep is also termed quiet sleep. Non-REM is further subdivided into 3 stages of progression:
- Stage 1 (light sleep)
- Stage 2 (so-called true sleep)
- Stage 3 to 4 (deep "slow-wave" or delta sleep)
With each descending stage, awakening becomes more difficult. It is not known what governs Non-REM sleep in the brain. A balance between certain hormones particularly growth and stress hormones may be important for deep sleep.
Rapid Eye-Movement Sleep (REM)
REM sleep is termed active sleep. Most vivid dreams occur in REM sleep. REM-sleep brain activity is comparable to that in waking, but the muscles are totally relaxed, possibly preventing people from acting out their dreams. In fact, except for vital organs like lungs and heart, the only muscles not relaxed during REM are the eye muscles. REM sleep may be critical for learning and for day-to-day mood regulation. When people are sleep-deprived, their brains must work harder than when they are well-rested.
The REM/Non-REM Cycle
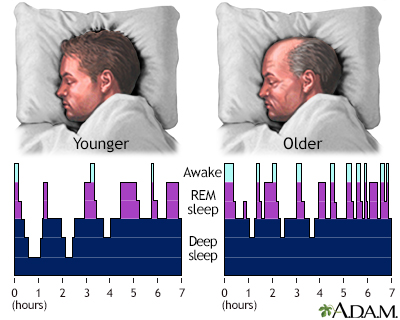
The cycle between quiet (non-REM) and active (REM) sleep generally follows this pattern:
- After about 90 minutes of non-REM sleep, eyes move rapidly behind closed lids, signifying REM sleep.
- As sleep progresses the non-REM/REM cycle repeats.
- With each cycle, non-REM sleep becomes progressively lighter, and REM sleep becomes progressively longer, lasting from a few minutes early in sleep to perhaps an hour at the end of the sleep episode.
Narcolepsy in the Pediatric Population
Symptoms of narcolepsy in children can vary from those seen in adults. Manifestations such as movement disorders or behavioral problems can make narcolepsy difficult to identify. Impaired school performance can be severe and can require special accommodations.
Causes
Genetic Factors
Narcolepsy has a genetic component and tends to run in families. An estimated 8% to 10% of people with narcolepsy have a close relative who has the disorder. An individual with a family member who has narcolepsy is 20 to 40 times more likely to have narcolepsy, compared to a person with no family history of the disease.
Researchers are looking for specific genetic mutations that may make individuals susceptible to this disorder, and have discovered that most affected individuals carry the HLA-DQB1*06:02 gene. More studies also show that the TCR-alpha gene, which interacts with the HLA genes, is also involved in narcolepsy.
However, genetics are not the only factor involved in narcolepsy. Narcolepsy most likely involves a combination of genetics and one or more environmental triggers, such as infection, trauma, hormonal changes, immune system problems, or stress.
Autoimmunity
Recent evidence suggests that narcolepsy may be an autoimmune disease, in which the immune system may be tricked into perceiving its own proteins to be antigens. Antigens are foreign substances targeted for attack by immune factors in the body.
In some diseases, the immune system overproduces potent factors called cytokines, which cause inflammation and injury in the susceptible cells and tissues affected by the disease. Most autoimmune diseases also tend to afflict those with particular subgroups of molecules of the immune system called human leukocyte antigens (HLAs).
Research suggests that an immune attack in narcolepsy may occur against cells containing the brain chemical, hypocretin (orexin). Hypocretin deficiency induces sleepiness and is present in around 90% of people with narcolepsy type 1. Studies have shown a reduced amount of hypocretin-positive neurons (nerve cells) in a vast majority of people with narcolepsy with cataplexy. Hypocretin deficiencies might set off chemical responses that produce sleep attacks.
Some HLAs, particularly the above-mentioned subgroup known as HLA-DQB1*06:02, have been strongly associated with narcolepsy and low levels of hypocretin. Because of the association between HLA-DQB1*06:02 and narcolepsy, an autoimmune basis is suspected to have some role in causing the disease. People with narcolepsy who carry this HLA group tend to have a specific collection of symptoms that include cataplexy and periodic limb movement disorder. However, roughly 20% of people without narcolepsy also carry these HLA types.
Risk Factors
Narcolepsy affects about 1 in 2,000 people. Experts estimate that around 135,000 to 200,000 Americans have narcolepsy, but the number may be higher. Only about half of people who have narcolepsy are actually diagnosed with the disorder. People are often mistakenly diagnosed with other conditions, such as psychiatric or emotional problems. Many people wait decades before receiving a proper diagnosis.
Age
Narcolepsy symptoms usually first appear in adolescence or young adulthood. While narcolepsy can begin at any age, symptoms typically first appear before the age of 25 and almost all patients are affected by age 35. Growing evidence suggests that the disorder may emerge in early childhood in many patients. It can often be misdiagnosed as another disorder, such as ADHD or depression. People who develop it at a young age often have a family history of the disease and a severe condition, suggesting that genetic factors are important in this group.
Complications
Narcolepsy is a life-long problem, but it is not progressive. Symptoms may even lessen over time, but they never completely disappear. In older adults, cataplexy may lessen over time, but sleep disturbances at night may worsen.
Risk for Accidents
Perhaps the most serious consequence of narcolepsy is the high risk for accidents. Multiple studies reported an increased risk for motor vehicle accidents for people with untreated narcolepsy. On the other hand, treating narcolepsy has been found to reduce this risk. For this reason, several countries prohibit people with narcolepsy from getting a driver's license, either indefinitely or until their condition is medically treated. Other common narcolepsy-related accidents include burns from touching hot objects, cuts from sharp objects, and breaking things.
Effects on Mental Functioning
Some studies report that people with narcolepsy have problems with memory, thinking, and attention. Whether these problems are more likely to be due to tiredness and episodes of sleepiness than to brain abnormalities is not clear.
Emotional and Social Difficulties
People with narcolepsy suffer emotional and social difficulties caused by their uncontrollable sleep episodes and cataplexy. Rates of depression in people with narcolepsy can range from 15% to 37%. (In the general population, the prevalence of major depression is 8%.) People may suffer from severe emotional and social dysfunction in all areas, including work, relationships, and leisure activities. Men with narcolepsy frequently suffer from sexual problems. Some experts believe that the psychological and social effects are more serious than those caused by epilepsy (for which narcolepsy can be mistaken).
Accompanying Physical Problems
Obesity
People with narcolepsy are at high risk for developing obesity compared to the general population. This could be a consequence of low activity level, but research also indicates that deficiencies in the brain chemical hypocretin may play a role in both narcolepsy and eating behaviors that could increase the risk for obesity.
Diagnosis
Although narcolepsy is a physical disorder, doctors are still very likely to misdiagnose people as having psychological problems. In most cases, narcolepsy is not diagnosed for years after the symptoms began. Sleep habits are not something typically asked about in a wellness visit. Today, there is no standard screening protocol for primary care doctors to detect sleep disorders. To determine specific sleep disorders, the doctor will take a medical and family history. The person should tell the doctor about any medications they are taking. The symptoms of narcolepsy are relatively easy to recognize if a person reports all of the major symptoms:
- Excessive daytime sleepiness with a tendency for frequent naps. These frequent naps should occur every day for at least 3 months to suggest the diagnosis of narcolepsy. Narcolepsy is usually diagnosed in adolescence and young adulthood when falling asleep suddenly in school brings the problem to attention.
- Cataplexy.
- Hypnagogic hallucinations.
- Sleep paralysis.
Diagnosis based only on symptoms, however, is often problematic for various reasons:
- People often seek medical help for single symptoms (sleep paralysis or hypnagogic hallucinations) that might be associated with other disorders, particularly epilepsy.
- Symptoms are sometimes not dramatically apparent for years, even to the person or a skilled observer. In some cases, the person may need to consult a sleep specialist or go to an accredited sleep disorder center for accurate diagnosis of a sleep disorder. People should carefully investigate centers to make sure that they offer full sleep studies. People who visit a sleep center undergo an in-depth analysis, usually supervised by a multidisciplinary team of consultants who can provide both physical and psychiatric evaluations.
Measurements of hypocretin-1 in the cerebrospinal fluid may be used in identifying difficult to diagnose cases of narcolepsy, since hypocretin is often absent in people with the condition. These include children below the age of 5 to 6 years and when the person is receiving anti-depressant medications that cannot be stopped.
Criteria
The current American Psychiatric Association diagnostic guidelines (DSM-5) require the presence of EDS for a narcolepsy diagnosis. This is defined as periods of feeling an irrepressible need to sleep or lapsing into sleep recurring multiple times within the same day, at least 3 days per week in the last 3 months. One of the following criteria must also be present:
- Episodes of cataplexy, occurring at least a few times per month (in narcolepsy type 1).
- Hypocretin deficiency. Hypocretin is measured in the cerebrospinal fluid (CSF).
- Abnormal sleep test results on either a nocturnal sleep polysomnography (PSG) or a multiple sleep latency test (MSLT).
Questionnaires
A doctor may administer certain questionnaires on sleeping habits, such as the Stanford Sleepiness Scale or the Epworth Sleepiness Scale.
The Epworth Sleepiness Scale (ESS)
The ESS uses a simple questionnaire to measure excessive sleepiness and differentiate it from normal daytime sleepiness.
Polysomnography
An overnight sleep study, called polysomnography (PSG), can be a valuable means for determining the basic cause of sleepiness. The person arrives at the sleep center about 2 hours before bedtime without having made any changes in daily habits. The person will be monitored by a variety of devices while sleeping:
- Electroencephalogram, or EEG, (monitors the electrical activity of the brain)
- Electrocardiogram, or ECG, (monitors the electrical activity of the heart)
- Electromyogram (monitors the movements of muscles)
- Electrooculogram (monitors eye movements)
- Pulse oximetry (monitors oxygen levels)
These instruments record activity as the person passes, or fails to pass, through the various sleep stages. A person with narcolepsy will have a nocturnal sleep polysomnography showing rapid eye movement (REM) sleep latency of 15 minutes or less.
Multiple Sleep Latency Test
The multiple sleep latency test (MSLT) uses a machine that measures the time it takes to fall asleep lying in a quiet room during the day. The patient takes 4 or 5 scheduled naps 2 hours apart. People with healthy sleep habits fall asleep in about 10 to 20 minutes. In patients with narcolepsy, PSG (see above) plus MSLT will show a much shorter duration of time (fewer than 8 minutes) from wakefulness into sleep. At least 2 of the naps are REM-onset (the active sleep phase associated dreaming). The PSG is usually performed before the MSLT, in order to ensure the patient has a good night's sleep and to exclude other sleep disorders. However, the test has limitations. There is no clear definition of exactly which abnormal results would indicate narcolepsy. It is most useful for measuring the severity of the problem. The Epworth Sleepiness Scale may be more accurate in differentiating narcolepsy from normal daytime sleepiness.
Laboratory Tests
Since narcolepsy with cataplexy (narcolepsy type 1) is caused in most cases by a hypocretin deficiency, laboratory measurements of hypocretin in the cerebrospinal fluid (CSF) are sometimes considered for a positive diagnosis of that disorder. Narcolepsy without cataplexy is usually associated with normal hypocretin levels, so diagnosis typically has to rely on only symptoms and sleep test results.
A genetic test to detect carriers of HLA-DQB1*0602 may also be considered in some cases. This variation is present in most patients with narcolepsy type 1 and in about 50% of patients with narcolepsy type 2. However, HLA-DQB1*0602 is also present in the general population. Therefore its presence does not necessarily confirm the narcolepsy diagnosis. A negative result however may be used to exclude narcolepsy in some people with cataplexy that may be caused by other conditions (such as brain lesions or multiple sclerosis).
Ruling out Other Sleep Disorders
The following sleep disorders can share some or all of the symptoms of narcolepsy:
-
Obstructive sleep apnea is associated with sleep disturbance and excessive daytime fatigue. A person may have both sleep apnea and narcolepsy.
Obstructive sleep apnea
An in-depth report about the causes, diagnosis, treatment, and prevention of obstructive sleep apnea.
Read Article Now Book Mark Article - Idiopathic hypersomnia is a less well-defined syndrome in which people have excessive daytime sleepiness without evidence of cataplexy. People have a hard time becoming fully awake despite an adequate amount of sleep.
-
Insomnia. Chronic sleep deprivation and inadequate sleep hygiene may be confused with the EDS of narcolepsy.
Insomnia
An in-depth report on the causes, diagnosis, treatment, and prevention of insomnia.
Read Article Now Book Mark Article - Secondary narcolepsy, resulting from head trauma, tumors, vascular malformations in the brain, multiple sclerosis, or Parkinson disease.
Multiple sclerosis
An in-depth report on the causes, diagnosis, and treatment of MS.
 Image
ImageRead Article Now Book Mark Article Parkinson disease
An in-depth report on the causes, diagnosis, and treatment of Parkinson disease.
Read Article Now Book Mark Article
Ruling out Psychological Disorders
Many people who have narcolepsy may be diagnosed incorrectly with some psychological or psychiatric problem. Certainly, people with narcolepsy have emotional difficulties because of the condition, and it is often difficult, particularly for a nonspecialist, to detect the physical problem. Even worse, hypnagogic hallucinations may result in diagnoses of schizophrenia or bipolar disorder, which are treated with potent antipsychotic drugs that have severe side effects and are useless for narcolepsy.
Ruling out Epilepsy
Narcolepsy can easily be mistaken for epilepsy, a group of disorders that cause seizures. Case studies have reported a misdiagnosis of epilepsy in people who were actually experiencing cataplexy and sleep paralysis. Electroencephalography (EEG) can determine if there is abnormal brain electrical activity to suggest underlying epilepsy. Some patients with epilepsy can also have narcolepsy.
Other Causes of Persistent Fatigue
A number of conditions can cause persistent fatigue and should be ruled out, including chronic fatigue syndrome. Other medical conditions, such as thyroid disease, can cause excessive daytime sleepiness as well and can often be excluded with simple blood tests.
These conditions may also worsen sleep paralysis in narcolepsy. Narcolepsy-associated sleep paralysis usually occurs at the onset of sleep and is chronic.
Treatment
Lifestyle treatment of narcolepsy includes taking three or more scheduled naps throughout the day and maintaining a regular sleep-wake schedule. People should also avoid heavy meals, caffeine-containing beverages, and alcohol before bedtime, as they can interfere with sleep.
People with mild narcolepsy symptoms who do not need medication may be able to maintain alertness with sleep scheduling. The role of scheduled naps for people who are responding to medications for narcolepsy remains unclear.
Medications for narcolepsy target the major symptoms of sleepiness and cataplexy. Stimulant drugs are used to reduce excessive daytime sleepiness while antidepressants and other drugs address cataplectic symptoms. The Food and Drug Administration (FDA) has approved three drugs specifically for the treatment of narcolepsy. They are now the first-line treatments:
- Modafinil (Provigil) and armodafinil (Nuvigil). For EDS.
- Sodium oxybate (Xyrem). For cataplexy and EDS.
Drug Treatments for Sleepiness
Modafinil
Modafinil (Provigil) is a drug used to treat the excessive sleepiness associated with narcolepsy and other sleep disorders. It has largely replaced methylphenidate (Ritalin) and other stimulants for treatment of narcolepsy sleepiness. People who switch to modafinil from stimulants such as methylphenidate have few problems if they gradually taper off the stimulant dose.
Dosage for adults ranges from 100 to 200 mg/day, usually taken once in the morning. Doses up to 400 mg/day (sometimes in 2 divided doses) may be used in some situations.
Modafinil helps people with narcolepsy stay awake during the day. While only some experience normal wake times, patients taking modafinil often have up to a 50% improvement in the ability to stay awake, as well as a 25% reduction in the number of involuntary sleep episodes. Modafinil is not recommended in pregnant women. Pregnant women or those wishing to get pregnant should discuss the risks and benefits of this medication with their doctors.
Some of modafinil's additional benefits include what it does not do:
- Modafinil does not appear to affect natural hormones important in sleep, including cortisol (the major stress hormone), melatonin, and growth hormone. Therefore, studies suggest that it does not interfere with voluntary naps during the day or with the quantity or quality of nighttime sleep.
- It does not cause anxiety to the degree that the standard stimulants do, but it can trigger psychiatric side effects, especially in people with previous mental disorders.
- It does not cause a rebound effect as stimulants do. In other words, people who take modafinil do not usually "crash" when the drug wears off.
- It has less potential for abuse than stimulant drugs. However, modafinil can still be habit-forming. People may need to gradually lower the dose before stopping treatment.
Side effects of modafinil may include:
- Headache (the most commonly reported side effect).
- Nausea.
- Diarrhea.
- Dry mouth.
- Nasal and throat congestion.
- Nervousness and anxiety.
- Dizziness.
- Back pain
- Difficulty sleeping.
- Decreases in the effects of hormonal methods of birth control, including the pill. (Women of childbearing age who take modafinil should switch to another form of birth control.)
- Modafinil is approved only for adults and should not be given to children.
Armodafinil (Nuvigil) is a newer drug, which is nearly identical to modafinil. In clinical trials comparing it with placebo, armodafinil improved wakefulness, memory, attention, and fatigue in people with narcolepsy.
Drug Warning
The FDA has added safety information to the prescribing label of modafinil (Provigil) and armodafinil (Nuvigil). The information warns that:
- Rare but serious skin reactions, such as Stevens-Johnson syndrome, have been reported with modafinil and armodafinil use. People should stop taking these medications at the first signs of any rash, and immediately contact their doctors.
- Psychiatric side effects, such as anxiety, mania, hallucinations, and suicidal thinking, have been reported. Doctors should be cautious about prescribing modafinil and armodafinil to people with a history of psychosis, depression, or mania.
Stimulants
Medications that act as stimulants used to be standard treatments for narcolepsy. They include:
- Methylphenidate (Ritalin)
- Dextroamphetamine (Dexedrine)
- Methamphetamine (Desoxyn)
The effects of methylphenidate and dextroamphetamine last for 2 to 5 hours. These drugs used to be considered useful for people who can manage wakefulness with a night's sleep and scheduled naps. They can improve mood, mental acuity, and other aspects of mental functioning. However, the evidence to support their benefit for people with narcolepsy is not as strong as with modafinil.
Stimulants have a high abuse potential and therefore their use should be closely monitored.
Stimulants can have unpleasant side effects, including:
- Weight loss
- Dizziness
- Nausea
- Changes in blood pressure and rapid heartbeat
- Headache
People with heart disease, hyperthyroidism, glaucoma, anxiety disorder, and high blood pressure should avoid stimulants, or take them only with a doctor's supervision.
These drugs become ineffective if used continuously, and people are advised to take a drug holiday one day a week or to withdraw gradually and resume treatment at a lower dose. People should not engage in activities that require mental alertness, such as driving, during withdrawal.
Some people with narcolepsy can schedule short naps throughout the day to help with symptoms of fatigue.
Pitolisant
Pitolisant (Wakix) is a drug that acts on the histamine receptor 3 (H3) to increases the production and release of histamine. In the brain, histamine acts as a neurotransmitter to promote wakefulness. Pitolisant was approved by the FDA in 2009 for the treatment of EDS in adult patients with narcolepsy. It is given as a pill once daily in the morning. Adverse effects include insomnia, nausea, and anxiety.
Drug Treatments for Cataplexy
Sodium oxybate (Xyrem)
Sodium oxybate (Xyrem), also referred to as gamma-hydroxybutyrate (GHB), helps reduce the frequency of cataplexy attacks and improve daytime sleepiness. People need to take GHB for about 4 weeks before they notice significant benefits. It may take an additional 4 weeks for the drug to reach maximum effect. Food intake can affect the actions of GHB, so people are advised to take it at a regular time after the evening meal.
Xyrem is a controlled substance. The FDA has placed tight restrictions on the use of this drug. Xyrem and the generic form of sodium oxybate can only be prescribed and dispensed under an FDA program called risk evaluation and mitigation strategy (REMS). Although the drug appears to be effective and safe when used for narcolepsy, it has a history of illegal and "date-rape" use, with street names such as "Grievous Bodily Harm" or "Liquid Ecstasy." (Despite this name, GHB is not the same as "Ecstasy," a street drug with different effects.) GHB can cause dependence over time. Education through the Xyrem Success Program may be valuable to people with narcolepsy and physicians.
Very serious side effects, including seizures, coma, respiratory arrest, and death, have been reported in people who abused GHB. However, clinical trials of Xyrem have not reported these effects with the doses used in treatment for cataplexy. Patients should be monitored closely for depression and suicidal thoughts, which may be worsened by use of sodium oxybate.
Because typical daily doses of sodium oxybate have a high sodium content, daily sodium intake amounts might be too high. Patients with heart disease, high blood pressure, and kidney disease should be monitored. A new oxybate drug containing less sodium is currently being investigated.
Antidepressants
Antidepressant drugs are not approved for treatment of cataplexy, but they are sometimes used to manage this condition. Unfortunately, there have been few studies conducted on antidepressant treatment of cataplexy, and there are little data on which type of antidepressant works bests. A comprehensive review has revealed that there is little to no evidence of any effectiveness for antidepressants in treating narcolepsy with regard to symptoms or quality of life.
Despite the lack of good evidence for their efficacy, antidepressants that continue to be used for cataplexy, hallucinations, sleep paralysis, and management of REM symptoms include:
- Tricyclic antidepressants. Protriptyline (Vivactil), clomipramine (Anafranil), imipramine (Janimine, Tofranil), and desipramine (Norpramin, Pertofrane).
- Selective serotonin reuptake inhibitors (SSRIs). Fluoxetine (Prozac), paroxetine (Paxil), and sertraline (Zoloft).
- Newer antidepressants. Venlafaxine (Effexor).
Tricyclics were the first antidepressants used for cataplexy; they were also one of the first treatments for cataplexy. They can be helpful for some people but have many unpleasant side effects, including dry mouth, constipation, and weight gain. Tricyclics can also lower blood pressure and cause disturbances in heart rhythm.
SSRIs have fewer side effects than tricyclics but may not work as well for cataplexy control. The most common side effects include nausea, drowsiness or insomnia, headache, weight gain, and sexual dysfunction.
Venlafaxine (Effexor) is a selective serotonin and norepinephrine reuptake inhibitor (SNRI) that has shown promising results for treatment of cataplexy. Some people with narcolepsy, and their doctors, report that venlafaxine seems to work best of all the antidepressants.
Monoamine Oxidase Inhibitors (MAOIs)
Selegiline (Eldepryl), also known as deprenyl, is an inhibitor of monoamine oxidase B (MAO). MAO is an enzyme that degrades dopamine, an important neurotransmitter. MAOIs may play a role in narcolepsy, but how much benefit this group of drugs provides is not well-proven. Selegiline is not FDA-approved for treatment of narcolepsy.
Selegiline has significant side effects. It interacts with nearly every antidepressant. People suffering from depression should discuss all treatment options with their doctor.
Depression
An in-depth report on the causes, diagnosis, treatment, and prevention of depression.

| Read Article Now | Book Mark Article |
People taking any MAOIs are at risk for high blood pressure if they consume tyramine-containing foods or beverages, including aged cheeses, most red wines, vermouth, dried meats and fish, canned figs, fava beans, and concentrated yeast products.
Researchers are using the recent knowledge on the causes of narcolepsy to design new therapies. Some treatments currently studied include administration of hypocretin, gene therapy, and immunotherapy. Treatments targeting the immune system offer promising therapy in the future but currently, there is insufficient evidence for such to support treatment outside of clinical trials.
Resources
- American Academy of Sleep Medicine -- aasm.org
- National Sleep Foundation -- www.thensf.org/
- Narcolepsy Network -- narcolepsynetwork.org
- Stanford Center For Narcolepsy -- med.stanford.edu/narcolepsy.html
- National Center on Sleep Disorders Research -- www.nhlbi.nih.gov/about/scienfic-divisions/national-center-sleep-disorders-research
- National Institute on Neurological Disorders and Stroke -- www.ninds.nih.gov
- Narcolepsy patient support -- www.morethantired.com
References
Abad VC, Guilleminault C. New developments in the management of narcolepsy. Nat Sci Sleep. 2017;9:39-57. PMID: 28424564 pubmed.ncbi.nlm.nih.gov/28424564.
Babiker MO, Prasad M. Narcolepsy in children: a diagnostic and management approach. Pediatr Neurol. 2015;52(6):557-565. PMID: 25838042 pubmed.ncbi.nlm.nih.gov/25838042.
Berry RB, Wagner MH. Modafinil and narcolepsy. In Berry RB, Wagner MH, eds. Sleep Medicine Pearls. 3rd ed. Philadelphia, PA: Elsevier Saunders; 2015:chap 91.
Cao MT, Guilleminault C. Narcolepsy: diagnosis and management. In: Kryger M, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 6th ed. Philadelphia, PA: Elsevier; 2017:chap 90.
Chokroverty S, Avidan AY. Sleep and its disorders. In: Daroff RB, Jankovic J, Mazziotta JC, Pomeroy SL, eds. Bradley's Neurology in Clinical Practice. 7th ed. Philadelphia, PA: Elsevier; 2016:chap 102.
Dye TJ, Gurbani N, Simakajornboon N. Epidemiology and pathophysiology of childhood narcolepsy. Paediatr Respir Rev. 2018;25:14-18. PMID: 28108192 pubmed.ncbi.nlm.nih.gov/28108192.
Flygare J, Parthasarathy S. Narcolepsy: Let the patient's voice awaken us! Am J Med. 2015;128(1):10-13. PMID: 24931392 pubmed.ncbi.nlm.nih.gov/24931392.
Golden EC, Lipford MC. Narcolepsy: Diagnosis and management. Cleve Clin J Med. 2018;85(12):959–969. PMID: 30526757 pubmed.ncbi.nlm.nih.gov/30526757.
Gupta R, Pandi-Perumal SR, Almeneessier AS, BaHammam AS. Hypersomnolence and traffic safety. Sleep Med Clin. 2017;12(3):489-499. PMID: 28778244 pubmed.ncbi.nlm.nih.gov/28778244.
Jain SV, Kothare SV. Disorders of excessive sleepiness. In: Swaiman KF, Ashwal S, Ferriero DM, et al, eds. Swaiman's Pediatric Neurology. 6th ed. Elsevier; 2017:chap 88.
Kornum BR, Knudsen S, Ollila HM, et al. Narcolepsy. Nat Rev Dis Primers. 2017;3:16100. PMID: 28179647 pubmed.ncbi.nlm.nih.gov/28179647.
Kotagal S. Narcolepsy. In Sheldon SH, Ferber R, Kryger MH, Gozal D, eds. Principles and Practice of Pediatric Sleep Medicine. 2nd ed. Philadelphia, PA: Elsevier Saunders; 2014:chap 18.
Liblau RS, Vassalli A, Seifinejad A, Tafti M. Hypocretin (orexin) biology and the pathophysiology of narcolepsy with cataplexy. Lancet Neurol. 2015;14(3):318-328. PMID: 25728441 pubmed.ncbi.nlm.nih.gov/25728441.
Lopez R, Barateau L, Evangelista E, Dauvilliers Y. Depression and hypersomnia: A complex association. Sleep Med Clin. 2017;12(3):395-405. PMID: 28778237 pubmed.ncbi.nlm.nih.gov/28778237.
Maski K, Owens JA. Insomnia, parasomnias, and narcolepsy in children: clinical features, diagnosis, and management. Lancet Neurol. 2016;15(11):1170–1181. PMID: 27647645 pubmed.ncbi.nlm.nih.gov/27647645.
Mignot E. Narcolepsy: genetics, immunology, and pathophysiology. In: Kryger M, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 6th ed. Philadelphia, PA: Elsevier; 2017:chap 89.
National Institute of Neurological Disorders and Stroke website. Narcolepsy fact sheet. www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Narcolepsy-Fact-Sheet. Updated August 13, 2019. Accessed January 30, 2020.
Owens JA. Sleep medicine. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21th ed. Philadelphia, PA: Elsevier; 2020:chap 31.
Partinen M, Kornum BR, Plazzi G, Jennum P, Julkunen I, Vaarala O. Narcolepsy as an autoimmune disease: the role of H1N1 infection and vaccination. Lancet Neurol. 2014;13(6):600-613. PMID: 24849861 pubmed.ncbi.nlm.nih.gov/24849861.
Plazzi G, Clawges HM, Owens JA. Clinical Characteristics and Burden of Illness in Pediatric Patients with Narcolepsy. Pediatr Neurol. 2018;85:21-32. PMID: 30190179 pubmed.ncbi.nlm.nih.gov/30190179.
Szabo ST, Thorpy MJ, Mayer G, Peever JH, Kilduff TS. Neurobiological and immunogenetic aspects of narcolepsy: Implications for pharmacotherapy. Sleep Med Rev. 2019;43:23-36. PMID: 30503715 pubmed.ncbi.nlm.nih.gov/30503715.
Taheri S. The immune basis of narcolepsy: What is the evidence? Sleep Med Clin. 2017;12(3):279-287. PMID: 28778227 pubmed.ncbi.nlm.nih.gov/28778227.
Thorpy MJ, Bogan RK. Update on the pharmacologic management of narcolepsy: mechanisms of action and clinical implications. Sleep Med. 2020;68:97-109. PMID: 32032921 pubmed.ncbi.nlm.nih.gov/32032921.
Vaughn BV, Basner RC. Sleep disorders. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier Saunders; 2020:chap 377.
Review Date: 3/31/2020
Reviewed By: Joseph V. Campellone, MD, Department of Neurology, Cooper Medical School at Rowan University, Camden, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.