
Ulcerative colitis - InDepth
Inflammatory bowel disease - ulcerative colitis - InDepth; Colitis - ulcerative - InDepth; IBD - ulcerative colitis - InDepth; Colitis - InDepth; Proctitis - InDepth; Ulcerative proctitis - InDepthAn in-depth report on the causes, diagnosis, treatment, and prevention of ulcerative colitis.
Highlights
Ulcerative Colitis
Ulcerative colitis and Crohn disease are inflammatory bowel diseases that cause chronic inflammation in the digestive system. Ulcerative colitis occurs only in the inner lining of the large intestine (colon) and rectum whereas Crohn disease extends into deeper areas of the intestinal wall and can affect any part of the gastrointestinal tract (digestive system).
Causes and Risk Factors
The exact causes of ulcerative colitis are unknown. Researchers observe that:
- Genetics plays some role. Many people with ulcerative colitis have family members with inflammatory bowel disease.
- Ulcerative colitis is diagnosed most often in people ages 15 to 35. However, it can occur at any age, including in older people.
- Ulcerative colitis is more common among whites than people of other races. Jewish people of Eastern European (Ashkenazi) descent have a higher than average risk of developing this disease.
Symptoms
The symptoms of ulcerative colitis depend in part on how widespread the disease is and the severity of the inflammation. Common symptoms include:
- Diarrhea
- Rectal bleeding
- Difficulty or pain when passing stool
- Abdominal cramps
- Bloody diarrhea
Prognosis
About one half of people with ulcerative colitis have mild symptoms while another half go on to develop more severe forms of the disease. Some people go into remission after a single attack, while others develop a chronic condition.
Treatment
The only cure for ulcerative colitis is surgical removal of the colon, but medications and dietary measures can help suppress the inflammatory response and control symptoms. Drugs used to treat ulcerative colitis include aminosalicylates (5-ASAs), corticosteroids, immunosuppressants, and biologic drugs. Some people with ulcerative colitis are not helped by drugs and require surgical treatment.
Introduction
Inflammatory bowel disease (IBD) is a general term that includes two main disorders:
- Ulcerative colitis
- Crohn disease
These two diseases are related, but they are considered separate disorders with somewhat different treatment options. The basic distinctions between UC and CD are location and severity. However, some people with early-stage IBD have features and symptoms of both disorders. (This is called indeterminate colitis.)
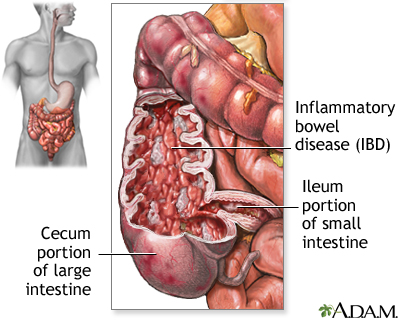
Crohn disease is an inflammation of the intestines. It often affects the ileum, the lower end of the small intestine, or even the entire small bowel as well as the colon. Ulcerative colitis is a similar inflammation of the colon or large intestine.
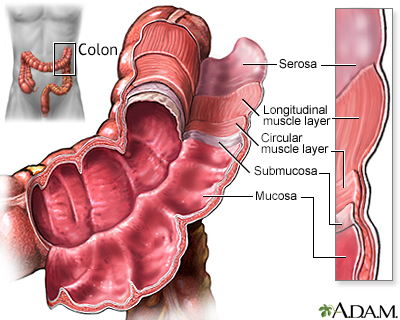
Ulcerative ColitisUlcerative colitis occurs only in the top layer of the large intestine (colon) and rectum. Ulcers form in the inner lining, or mucosa, of the colon or rectum, causing diarrhea, which may be accompanied by blood and pus.
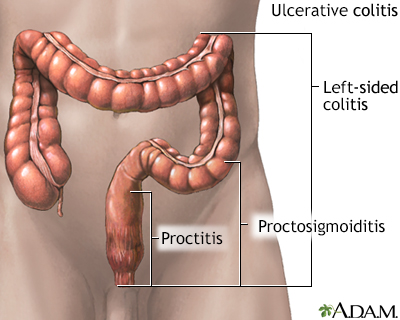
Ulcerative colitis is classified into different categories depending on the location of the disease. The four main types of ulcerative colitis are:
-
Proctitis.
Disease confined to the rectum (the lower part of the colon that connects with the anus). In about one third of people, ulcerative colitis begins with ulcerative proctitis. -
Proctosigmoiditis.
Disease that affects the rectum and the sigmoid colon (the lower part of the colon located above the rectum). -
Left-Sided Colitis.
Disease that causes continuous inflammation throughout the left side of the colon from the rectum to the area near the spleen. -
Pancolitis.
Disease and inflammation throughout the entire colon.
Crohn Disease
Crohn disease can occur in any part of the gastrointestinal tract (digestive system) from the mouth to the anus. The inflammation associated with Crohn disease affects all layers of the intestine and can extend into the deep layers of the intestinal wall.
The Gastrointestinal Tract
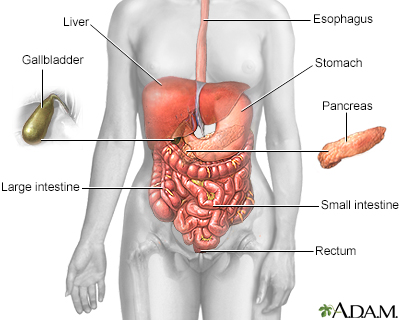
The gastrointestinal (GI) tract (the digestive system) is a tube that extends from the mouth to the anus. It is a complex organ system that first carries food from the mouth down the esophagus to the stomach and then through the small and large intestine to be excreted through the rectum and anus.
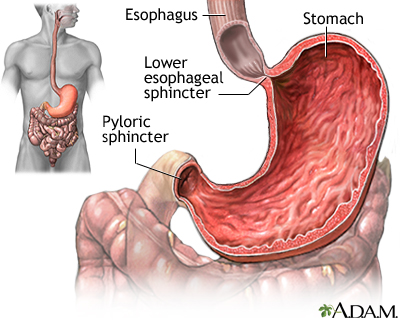
EsophagusThe esophagus, commonly called the food pipe, is a narrow muscular tube, about 9 1/2 inches (24 centimeters) long that begins below the tongue and ends at the stomach.
StomachIn the stomach, acids and stomach motion break food down into particles small enough so that nutrients can be absorbed by the small intestine.
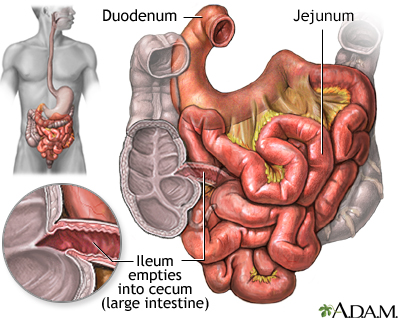
Small IntestineThe small intestine, despite its name, is the longest part of the gastrointestinal tract. It extends from the stomach to the large intestine and is about 6 m or 20 feet long. Food passes from the stomach through the small intestine's three parts:
- First it enters the
duodenum
- Then the
jejunum
- Finally the
ileum
Most of the digestive process occurs in the small intestine.
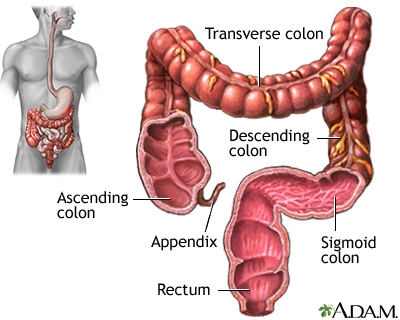
Large IntestineUndigested material, such as plant fiber, is passed next to the large intestine, or colon, mostly in liquid form. The colon is wider than the small intestine but only about 1.5 m or 6 feet long. The colon absorbs excess water and salts into the blood. The remaining waste matter is converted to feces through bacterial action. The colon is a continuous structure but it is characterized as having several components.Cecum and AppendixThe cecum is the first part of the colon. The appendix is attached to the cecum. These structures are located in the lower-right part of the abdomen. The colon continues onward in several sections:
- The first section, the
ascending colon
, extends upward from the cecum on the right side of the abdomen. - The second section, the
transverse colon
, crosses the upper abdomen to the left side. - The third section extends downward on the left side of the abdomen toward the pelvis and is called the
descending colon
. - The final section is the
sigmoid colon
.
Feces are stored in the descending and sigmoid colon until they pass through the rectum and anus. The rectum extends through the pelvis from the end of the sigmoid colon to the anus.
Causes
Doctors do not know exactly what causes inflammatory bowel disease. IBD appears to be due to an interaction of many complex factors including genetics, impaired immune system response, and environmental triggers.
The result is an abnormal immune system reaction, which in turn causes an inflammatory response in the body's intestinal regions. Ulcerative colitis and Crohn disease, like other IBDs, are considered autoimmune disorders.
The Inflammatory Response
An inflammatory response occurs when the body tries to protect itself from what it perceives as invasion by a foreign substance (antigen). Antigens may be viruses, bacteria, or other harmful substances.
In Crohn disease and ulcerative colitis, the body mistakenly targets harmless substances (food, beneficial bacteria, or the intestinal tissue itself) as harmful. To fight infection, the body releases various chemicals and white blood cells, which in turn produce byproducts that cause chronic inflammation in the intestinal lining. Over time, the inflammation damages and permanently changes the intestinal lining.
Genetic Factors
Genetic factors are certainly involved in IBD. A significant number of people with ulcerative colitis have family members with the same disease or Crohn disease. Several identified genes and chromosome locations play a role in the development of ulcerative colitis, Crohn disease, or both.
Genetic factors appear to be more important in Crohn disease, although there is evidence that both conditions have some genetic defects in common.
Environmental Factors
Inflammatory bowel disease is much more common in industrialized nations, urban areas, and northern geographical latitudes. It is not clear how or why these factors increase the risk for IBD.
It could be that "Western" lifestyle factors (smoking, exercise, diets high in fat and sugar, stress) play some role. However, there is no strong evidence that diet or stress cause Crohn disease or ulcerative colitis, although they can aggravate the conditions.
Risk Factors
About 1 million Americans suffer from inflammatory bowel disease (IBD). About one half of these people have ulcerative colitis. There are several risk factors for ulcerative colitis.
Age
Ulcerative colitis can occur at any age, but it is most often diagnosed in people ages 15 to 35 and, less commonly, in people ages 50 to 75.
Sex
Men and women are equally at risk for developing ulcerative colitis.
Family History
Ulcerative colitis tends to run in families. People who have a first-degree relative (father, mother, brother, sister) with ulcerative colitis have a significantly greater risk of developing the disorder.
Race and Ethnicity
Crohn disease and ulcerative colitis are more common among whites than people of other races. Jews of Eastern European (Ashkenazi) descent are at especially high risk. However, rates of inflammatory bowel disease have been increasing among other racial and ethnic groups.
Smoking
Smoking appears to decrease the risk of developing ulcerative colitis. (Smoking, however, should never be used to protect against ulcerative colitis.) Conversely, smoking increases the risk of developing Crohn disease and can worsen the course of the disease.
Appendectomy
Removal of the appendix (appendectomy) may possibly reduce the risk of developing ulcerative colitis but increase the risk for Crohn disease.
Symptoms
The two major inflammatory bowel diseases, ulcerative colitis and Crohn disease, share certain characteristics:
- Symptoms usually appear in young adults.
- Symptoms can develop gradually or have a sudden onset.
- Ulcerative colitis and Crohn disease are chronic conditions. In both diseases, people experience sporadic episodes of symptom flare-ups (relapse) in between symptom-free periods (remission).
- Symptoms can be mild or very severe. Severe symptoms can lead to complications.
Common Symptoms
The symptoms of ulcerative colitis depend in part on how widespread the disease is and the severity of the inflammation. Common symptoms include:
- Diarrhea
- Rectal bleeding and bloody stool
- Difficulty or pain when passing stool
- Abdominal cramps
Other symptoms may include:
- Fever
- Nausea
- Loss of appetite and weight loss
- Fatigue
Non-Intestinal Symptoms
The inflammation associated with inflammatory bowel disease (IBD) can cause symptoms outside of the gastrointestinal tract.
JointsArthritis is the most common non-intestinal symptom of inflammatory bowel disease.
Skin DisordersThere are many types of skin problems associated with IBD. They often tend to appear during disease flare-ups and resolve when symptoms are controlled. Canker sores (mouth ulcers) are very common. Skin disorders that tend to be seen more with ulcerative colitis than Crohn disease include, red knot-like swellings (erythema nodosum) and pus-filled skin ulcers on the shins and ankles (pyoderma gangrenosum).
EyesInflammatory bowel disease is sometimes associated with various eye problems. A common complication is inflammation in the pigmented part of the eye, a condition called uveitis.
Prognosis
About one half of people with ulcerative colitis have mild symptoms while another half go on to develop more severe forms of the disease. People with more severe ulcerative colitis tend to respond less well to medications.
The course of ulcerative colitis is unpredictable. Some people go into remission after a single attack, while others develop a chronic condition. The only cure for ulcerative colitis is surgical removal of the colon, but medications can help suppress the inflammatory response and control symptoms.
Complications
Complications in the Intestine
Malabsorption and MalnutritionMalabsorption is the inability of the intestines to absorb nutrients. In inflammatory bowel disease (IBD), this occurs as a result of bleeding and diarrhea, as a side effect from some of the medications, and as a result of surgery. Malnutrition may occur in ulcerative colitis, but it tends to be less severe than with Crohn disease.
Toxic MegacolonToxic megacolon is a serious complication that can occur if inflammation spreads into the deeper layers of the colon. In such cases, the colon enlarges and becomes paralyzed. In severe cases, it may rupture, which is a life-threatening event requiring emergency surgery. Symptoms include weakness, abdominal pain, abdominal distention, and frequently, fever.
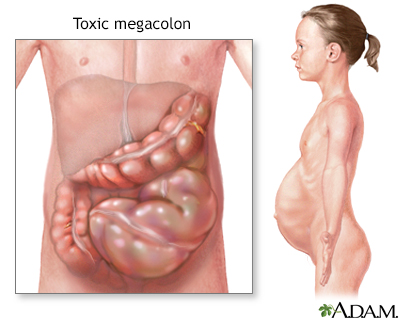
Toxic megacolon is characterized by extreme inflammation and distention of the colon. Common symptoms are pain, distention of the abdomen, fever, rapid heart rate, and dehydration. This is a life-threatening complication that requires immediate treatment, usually surgical removal of the colon.
Bleeding and AnemiaRectal bleeding due to ulcers in the colon is a common complication of ulcerative colitis. It can increase the risk for anemia (reduced red blood cell count). In some cases, internal bleeding can be massive and dangerous, requiring surgery.
Intestinal InfectionsInflammatory bowel disease can increase susceptibility to Clostridium difficile, a species of intestinal bacteria that causes severe diarrhea. It is usually acquired in a hospital. However, studies indicate that C difficile infection is increasing among people with IBD, including outside of hospital settings. People with ulcerative colitis are at particularly high risk.
Colorectal CancerInflammatory bowel disease increases the risk for colorectal cancer. The risk is highest for people who have had the disease for at least 8 years or who have extensive areas of colon involvement. The more severe the disease, and the more it has spread throughout the colon, the higher the risk. Having a family history of colorectal cancer also increases risk. If you have an IBD, discuss with your health care provider how often you should have a colonoscopy screening test for colorectal cancer.
Most guidelines recommend that people with IBD receive an initial colonoscopy earlier than people with no risk factors for colon cancer. Schedules for follow-up colonoscopies are based on various risk factors. Some of these risk factors include severity of ulcerative colitis disease, family history of colorectal cancer, presence of primary sclerosing cholangitis, personal history of abnormal cells (dysplasia) in the colon, and presence of colonic strictures.
Complications Outside the Intestine
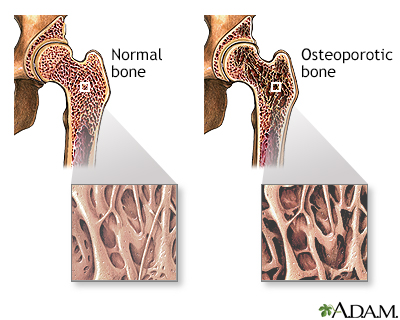
BonesUlcerative colitis, and the corticosteroid and immune-suppressing drugs used to treat it, can cause osteopenia (low bone density) and osteoporosis (bone loss). Osteoporosis is more common with Crohn disease than with ulcerative colitis.
Liver and Gallbladder Disorders
In severe cases, IBD can cause problems with the liver and pancreas and increase the risk for gallstones. In addition, patients with IBD are at increased risk of developing primary sclerosing cholangitis. This is a disease of the bile ducts in the liver that eventually leads to liver failure and the need for liver transplantation.
Thromboembolism (Blood Clots)People with inflammatory bowel disease are at higher risk for blood clots, especially deep venous thrombosis where blood clots form in the legs. They are also at risk for pulmonary embolism, when a blood clot travels from the legs to the lungs.
Urinary Tract and Kidney DisordersIBD may increase the risk for urinary tract and bladder infections. People with IBD have an increased risk for kidney stones.
Delayed Growth and Development in ChildrenChildren with ulcerative colitis are at slightly higher than average risk for delayed growth, but their risk is lower than with Crohn disease.
Emotional FactorsLiving with ulcerative colitis can pose many emotional challenges. Feelings of frustration, humiliation, and loss of control are common although symptoms can be emotionally stressful, and symptom flare ups are sometimes associated with stressful life events, there is no evidence that stress or psychological factors cause IBD.
Diagnosis
There is no definitive diagnostic test for ulcerative colitis. A health care provider will diagnose ulcerative colitis based on medical history and physical examination, and the results of laboratory, imaging, and endoscopic tests, which usually include biopsies of colon tissue.
Laboratory Tests
Blood tests are used for various purposes, including determining the presence of anemia (low red blood cell count). An increased number of white blood cells or elevated levels of inflammatory markers such as C-reactive protein may indicate the presence of inflammation.
An inflammatory bowel disease panel is a blood test that can help with diagnosis in certain people.
A stool sample may be taken and examined for blood, infectious organisms, or both.
A substance called fecal calprotectin can be found to increase in the stool of patients having a flare-up of their IBD.
Endoscopy
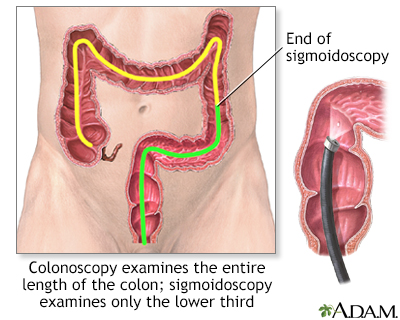
Flexible Sigmoidoscopy and ColonoscopyFlexible sigmoidoscopy and colonoscopy are standard endoscopic procedures for diagnosing ulcerative colitis. They are important in the diagnosis of both ulcerative colitis and Crohn disease. Both procedures involve snaking a flexible tube called an endoscope (videoscope) through the rectum to view the lining of the colon.
- Sigmoidoscopy, which is used to examine the rectum and left (sigmoid) colon, lasts about 10 minutes and is done without sedation. It may be mildly uncomfortable, but it is not painful. If sigmoidoscopy indicates ulcerative colitis, the doctor may order a colonoscopy to confirm the diagnosis and to identify how much of the colon is involved.
- Colonoscopy allows a view of the entire colon and requires a sedative, but it is still a painless procedure performed on an outpatient basis. A colonoscopy is also used to screen for colon cancer.
During these procedures, the doctor can insert instruments through the endoscope to remove tiny tissue samples (biopsies). A pathologist will view the tissue sample under a microscope to look for signs of inflammation.
These procedures can help distinguish between ulcerative colitis and Crohn disease, as well as other diseases. People diagnosed with ulcerative colitis may also need periodic endoscopies to evaluate their condition when symptoms flare up.
Other Imaging Tests
Sigmoidoscopy and colonoscopy are standard tests for diagnosing ulcerative colitis, but in some cases x-ray testing is used, especially to see the small intestine.
Other possible imaging tests include a special CT scan called a CT enteroscopy, an MRI called MR enteroscopy, a double contrast barium enema (rarely done), a small bowel x-ray series, and a swallowed capsule that is a camera, called wireless capsule endoscopy.
Ruling out Diseases Resembling Ulcerative ColitisCrohn DiseaseCrohn disease and ulcerative colitis can share similar symptoms. Ulcerative colitis tends to cause more rectal discomfort (tenesmus) and bleeding than Crohn. Fistulas (tracts between areas of the intestine, between the intestine and other organs, or between the intestine and the skin) and strictures (scarring) are common with Crohn disease but very rare with ulcerative colitis. Endoscopy and imaging tests reveal more extensive involvement through the entire gastrointestinal tract with Crohn disease than with ulcerative colitis. Ulcerative colitis only occurs in the colon and rectum.
Irritable Bowel SyndromeIrritable bowel syndrome (IBS), also known as spastic colon, functional bowel disease, and spastic colitis, may cause some of the same symptoms as inflammatory bowel disease (IBD). Bloating, diarrhea, constipation, and abdominal cramps are all symptoms of IBS. However, IBS is not the same as IBD in that it does not cause abnormalities to the lining of the intestine. Behavioral therapy may be helpful in treating IBS. (Psychological therapy does not improve inflammatory bowel disease.)
Infectious ColitisInfectious colitis appears very rapidly and painfully. Organisms can be identified in stool samples.
Intestinal Ischemia (Ischemic Colitis)Symptoms similar to irritable bowel syndrome can be caused by blockage of blood flow in the intestine. This is more likely to occur in elderly people.
Celiac SprueCeliac sprue, or celiac disease, is intolerance to gluten (found in wheat) that triggers inflammation in the small intestine and causes diarrhea, vitamin deficiencies, and stool abnormalities. It occurs in some people with inflammatory bowel disease (IBD).
Acute Appendicitis
Crohn disease may cause tenderness in the right lower part of the abdomen, where the appendix is located, that resembles appendicitis.
CancerColon or rectal cancers must always be ruled out when symptoms of IBD occur.
Treatment
Ulcerative colitis is a chronic condition marked by variable periods of no symptoms (remission) and active symptoms (flare-ups). Treatment can help suppress the inflammatory response and manage symptoms. A treatment plan for ulcerative colitis includes:
- Diet and nutrition
- Medications
- Surgery (when necessary)
Diet and Nutrition
Malnutrition may occur in ulcerative colitis, although it tends to be less severe and occurs less frequently than with Crohn disease. People with ulcerative colitis may experience reduced appetite and weight loss.
It is important to eat a well-balanced healthy diet and focus on getting enough calories, protein, and essential nutrients from a variety of food groups. These include protein sources, such as meat, chicken, fish or soy, dairy products, such as milk, yogurt, and cheese (if the patient is not lactose-intolerant), and fruits and vegetables. Depending on your nutritional status, your health care provider may recommend that you take a vitamin or iron supplement.
Medications
Drug therapy for ulcerative colitis aims to resolve symptoms (induce remission) and prevent flare-ups (maintain remission). These are discussed in more detail in the Medications section below. The main types of drugs used for treating ulcerative colitis are:Aminosalicylates.
Mild-to-moderate ulcerative colitis is usually treated with aspirin-like medications called aminosalicylates, or 5-ASAs. These drugs are also used to treat relapses.Corticosteroids.
Corticosteroids (steroids) may be used short-term for moderate-to-severe ulcerative colitis to treat flares and induce remission. Because of their significant side effects, they are not recommended for long-term use and maintenance therapy.Immunosuppressants.
Drugs that suppress the immune system (immunosuppressants) are useful, either alone or in combinations, to induce remission in milder cases of ulcerative colitis, or maintain remission in people who have been treated with steroids.Biologic Drugs.
Biologic drugs used for ulcerative colitis target and block specific proteins involved with the inflammatory response. They are used to induce or maintain remission in moderate-to-severe ulcerative colitis.
Drug therapy is considered successful if it can push the disease into remission (and keep it there) without causing significant side effects. A person's condition is generally considered in remission when the intestinal lining has healed and symptoms such as diarrhea, abdominal cramps, and tenesmus (straining painfully to defecate) are normal or close to normal.
Other types of drugs may also be used to treat specific conditions and symptoms associated with ulcerative colitis:
- Antibiotics may be used to treat bacterial overgrowth or complications like pouchitis.
- Certain probiotics are also helpful in pouchitis.
- Anti-diarrheal medications such as loperamide (Imodium, generic) may help control diarrhea but you should only use them if your health care provider says it is safe to do so.
Surgery
Drugs are not helpful in all cases of ulcerative colitis. As a result, some people need surgical treatment. Surgery may also be necessary because of a hemorrhage, perforation of the colon, or toxic megacolon.
Total proctocolectomy with ileal pouch anal anastomosis (IPAA), also known as restorative proctocolectomy, and total proctocolectomy with ileostomy are the two definitive surgical approaches for widespread ulcerative colitis that cannot be controlled with medications. Colectomy (resection of a portion of the colon) may be performed for more limited disease.
Unlike Crohn disease, which can recur after bowel resection, ulcerative colitis does not recur after total proctocolectomy. Total proctocolectomy is considered a cure for ulcerative colitis. (See the Surgery section for more detailed information.)Medications
Aminosalicylates
Aminosalicylates contain the compound 5-aminosalicylic acid, or 5-ASA, which helps reduce inflammation. These drugs are used to prevent relapses and maintain remission in mild-to-moderate ulcerative colitis.
5-ASA TypesThe standard aminosalicylate drug is sulfasalazine (Azulfidine, generic). This drug combines the 5-ASA drug mesalamine with sulfapyridine, a sulfa antibiotic. While sulfasalazine is inexpensive and effective, the sulfa component of the drug can cause unpleasant side effects, including headache, nausea, and rash.
People who cannot tolerate sulfasalazine or who are allergic to sulfa drugs have other options for aminosalicylate drugs, including mesalamine (Asacol, Pentasa, Lialda, Delzicol, generic), olsalazine (Dipentum), and balsalazide (Colazal, generic). These drugs, like sulfasalazine, are taken as pills several times a day. Lialda and Apriso are once-daily mesalamine pills for people with ulcerative colitis. Mesalamine is also available in enema (Rowasa, generic) and suppository (Canasa, generic) forms.
Side Effects of 5-ASAsSide effects of aminosalicylate drugs may include:
- Abdominal pain and cramps
- Diarrhea
- Gas
- Nausea
- Hair loss
- Headache
- Dizziness
Corticosteroids (commonly called steroids) are powerful anti-inflammatory drugs used to treat moderate-to-severe ulcerative colitis. Because long-term steroid use can cause significant side effects, corticosteroids are used only a short period of time with the goal of inducing remission.
Corticosteroid TypesPrednisone (Deltasone, generic), methylprednisolone (Medrol, generic), and hydrocortisone (Cortef, generic) are the most common oral corticosteroids. Budesonide (Entocort, Uceris, generic) is a newer type of steroid that is used as an alternative. Most oral steroids circulate through the body and have widespread side effects. Budesonide affects only local areas in the intestine and tends to have fewer side effects.
Administering CorticosteroidsMost corticosteroids can be taken as a pill. For people who cannot take oral forms, steroids may be given intravenously or rectally as a suppository, enema, or foam. The severity or location of the condition often determines the form.
Side Effects of CorticosteroidsCommon side effects of short-term treatment with oral steroids can include acne, increased appetite, and insomnia. Long-term treatment with steroids increases the risk for many serious side effects including low bone density (osteoporosis), high blood pressure, diabetes, and cataracts.
Withdrawing from CorticosteroidsOnce remission is achieved and the intestinal inflammation has subsided, steroids must be withdrawn very gradually. Withdrawal symptoms, including fever, malaise, and joint pain, may occur if the dosage is lowered too rapidly. If this happens, the dosage is increased slightly and maintained until symptoms are gone. More gradual withdrawal is then resumed. To maintain remission, people who are treated with steroids are given an immunomodulator or biologic drug.
Some people cannot stop taking steroids without having a relapse of their symptoms. They may be treated with immunomodulators or biologic drugs or be candidates for surgery.
Immunosuppressive Drugs (Immunomodulators)
Immunosuppressant drugs, also called immunomodulators, suppress or limit actions of the immune system and therefore the inflammatory response that causes ulcerative colitis. These drugs may be used in combination with a biologic drug to induce remission. They may also be used alone to maintain remission in people who were treated with steroid drugs. Immunosuppressants allow corticosteroids to be safely withdrawn. (Chronic steroid use is not desirable because of its side effects). For this reason, immunosuppressants are sometimes referred to as steroid-sparing drugs.
Immunomodulator TypesAzathioprine (Imuran, Azasan, generic) and mercaptopurine ([6-MP], Purinethol, generic) are the standard oral immunosuppressant drugs. They belong to a class of medications called thiopurines. Methotrexate (MTX, Rheumatrex) is another type of immunosuppressant that is used more often for Crohn disease but may be used in some cases for ulcerative colitis.
Other pill forms of immunosuppressants include cyclosporine A (Sandimmune, Neoral) and tacrolimus (Prograf). They may be used to treat people with very severe ulcerative colitis.
Side Effects of ImmunomodulatorsGeneral side effects of immunosuppressants may include:
- Nausea and vomiting
- Susceptibility to infections
- Liver or pancreatic inflammation
People who take these drugs should receive frequent blood tests to monitor white blood cell count and liver function. A serious concern associated with thiopurines is increased risk for lymphoma, a cancer that starts in the immune system.
Biologic Drugs
Biologic drugs are genetically engineered drugs to target specific proteins involved with the body's inflammatory response. Biologics are given to help induce and maintain remission.
Four biologic drugs are approved for treatment of moderate-to-severe ulcerative colitis in people who have not responded to other drugs:
- Infliximab (Remicade), which is given by intravenous (IV) infusion in a doctor's office or hospital clinic (after the first 3 doses, the drug is administered every 8 weeks).
- Adalimumab (Humira), which you can give by injection at home (after the first 2 doses, you give yourself an injection every other week).
- Golimumab (Simponi) is given by self-injection at home once a month.
- Vedolizumab (Entyvio) is given by IV infusion (after the first 3 doses, the drug is administered every 8 weeks).
- Ustekinumab (Stelara) first dose is given as an IV infusion in the doctor’s office or clinic. After the first dose, an injection is given every 8 weeks.
Infliximab, adalimumab, and golimumab target and block an inflammatory immune factor known as tumor necrosis factor (TNF). These drugs are called anti-TNF drugs or TNF blockers. Vedolizumab is an integrin receptor antagonist that works in a different way than anti-TNF drugs. It is approved for people with ulcerative colitis who were not helped by immunomodulators or anti-TNF drugs, or who are dependent on steroids. Ustekinumab targets the proteins interleukin-12 (IL-12) and interleukin 23 (IL-23).
Side Effects of BiologicsBiologic drugs can cause pain and swelling at the injection site. Other common side effects may include:
- Upper respiratory infections
- Headache
- Rash
- Stomach and back pain
- Nausea
Some people have allergic reactions to these drugs.
These drugs may increase the risk for infections, including tuberculosis and reactivation of hepatitis B. People need to be tested for these infections before starting treatment. Your health care provider should monitor you for any signs of viral, bacterial, or fungal infection. People who take biologic drugs should also receive regular tests for signs of problems. You will need frequent blood tests.
There is a concern that the anti-TNF drugs (infliximab, adalimumab) may increase the risk for lymphomas and leukemia cancers. However, recent studies have disputed these findings and the benefits of these drugs appear to outweigh the risks for cancer.
Vedolizumab may possibly increase the risk for a rare neurological condition called progressive multifocal leukoencephalopathy (PML), which can lead to death or severe disability.
Other DrugsTofacitinib (Xeljanz) was approved by the FDA as a long-term treatment for people with moderate-to-severe ulcerative colitis. Tofacitinib blocks a molecule called Janus kinase. It is given as a pill taken twice daily. The American College of Gastroenterology recommends tofacitinib for patients who previously failed anti-TNF therapy (like infliximab, adalimumab, and golimumab). Similar to anti-TNF drugs, tofacitinib can increase the risk for serious infections and malignancy.
Surgery
Proctocolectomy and Ileoanal Anastomosis
Proctocolectomy is removal of the entire colon, including the lower part of the rectum and the sphincter muscles that control bowel movements. It can achieve a complete cure, but it is a last resort for ulcerative colitis that has not been helped by drug therapy.
IleostomyIn some proctocolectomies, the surgeon creates an opening in the abdominal wall (called a stoma) to allow passage of waste material. This part of the procedure is referred to as an ileostomy. The stoma is created in the lower right corner of the abdomen. The surgeon then connects cut ends of the small intestine to this opening. An ostomy bag is placed over the opening and accumulates waste matter. It requires emptying several times a day.
Ileoanal AnastomosisIleal pouch anal anastomosis (IPAA), also simply called ileoanal anastomosis, has now largely replaced ileostomy because it preserves part of the anus and allows for more normal bowel movements. The procedure creates a natural pouch to collect waste, rather than using an ileostomy bag. The standard procedure involves:
- The colon is removed as in proctocolectomy, but the surgeon only strips the superficial diseased inner layer of the rectum, leaving the sphincter muscles intact.
- The anus is then attached to the ileum (the final portion of the small intestine leading to the colon).
- A pouch is constructed out of the small bowel above the anus. The pouch is able to collect waste material, and a person can pass bowel movements normally through the anus, although they are watery and more frequent than normal (5 to 6 times a day).
- A temporary abdominal opening (ileostomy) is usually required, but it is typically closed up in a second operation a few months later.
Managing Daily Life after Surgery
Flatulence (passing gas) is a common problem following surgery. People may need to avoid insoluble fiber foods, such as popcorn, olives, and vegetable skins, which can obstruct the stoma. Some pouching systems have filters that can help limit flatulence.
It is important to increase fluid intake, and include not only water but also broth, sports drinks, and vegetable juice to maintain appropriate levels of sodium and potassium.
Ileostomy and ileoanal anastomosis do not interfere with bathing or showering or most physical activity except for contact sports. As a rule, the surgeries do not impair sexual function.
Outcome and Complications from Ileoanal Anastomosis
Complications are common with any intestinal operation. In a small percentage of IPAA procedures, complications occur that require conversion to an ileostomy.
PouchitisInflammation of the pouch (pouchitis) is the most common complication of the pouch procedures. Symptoms include rectal bleeding, cramps, and fever. It can usually be successfully treated with antibiotics such as metronidazole (Flagyl, generic) or ciprofloxacin (Cipro, generic).
Bowel obstructionBowel obstruction may occur although it is less common than pouchitis. With most people, this condition can be treated by avoiding food for several days and administering intravenous fluids. In some cases of bowel obstruction, surgery may need to be performed to remove the blockage.
Pouch failurePouch failure occurs in a small percentage of people. It requires permanent removal of the pouch and use of ileostomy.
Irritable Pouch SyndromeIrritable pouch syndrome is a problem that includes frequent bowel movements, an urgent need to defecate, and abdominal pain. However, there are no signs of inflammation as there are with pouchitis. Stress and diet play a role in this condition, and it is usually relieved after a bowel movement.
InfertilityIPAA can cause infertility in women because the surgery can scar or block the fallopian tubes.
Lifestyle Changes
Diet and Nutrition
Certain types of foods may worsen diarrhea and gas symptoms, especially during times of active disease. While people vary in their individual sensitivity to foods, general guidelines for dietary management during symptom flare-ups include:
- Eat small amounts of food throughout the day.
- Stay hydrated by drinking lots of water (frequent consumption of small amounts throughout the day).
- Eat soft, bland foods and avoid spicy foods.
- Avoid high-fiber foods (bran, beans, nuts, seeds, and popcorn).
- Avoid fatty greasy or fried foods and sauces (butter, margarine, and heavy cream).
- Limit milk products if you are lactose intolerant (or consider taking a lactase supplement to improve tolerance). Otherwise, dairy products are a good source of protein, calcium, and vitamin D.
- Avoid or limit alcohol and caffeine consumption.
Dietary Supplements
Your health care provider may recommend you take a multivitamin. Although other types of dietary supplements, such as probiotics ("healthy bacteria" like lactobacilli) and omega-3 fatty acids have been investigated for ulcerative colitis, there is no conclusive evidence that they are effective in controlling symptoms or preventing disease relapses.
Be sure to tell your provider of any herbs or supplements you are taking or considering taking as some of these may be unsafe or interact with medications.
Pain Relievers
Some people have more symptoms after taking aspirin or non-steroidal anti-inflammatory medicines (NSAIDs) such as ibuprofen (Advil, generic) or naproxen (Aleve, generic). Some clinicians believe that the use of NSAIDs in patients with IBD can activate the disease. Ask your provider whether you can take these medicines.
Stress Management
Stress does not cause Crohn disease or ulcerative colitis, but it can trigger and worsen symptoms. Many people find that stress management techniques help them cope better with living with IBD. Stress management can include:
- Meditation
- Yoga and relaxation response training
- Getting adequate sleep
- Exercising regularly
- Building a healthy support network of family and friends
Some people may also benefit from psychological counseling.
Resources
- Crohn's & Colitis Foundation of America -- www.crohnscolitisfoundation.org
- American Gastroenterological Association -- www.gastro.org
- American College of Gastroenterology -- gi.org
- National Institute of Diabetes and Digestive and Kidney Diseases -- www.niddk.nih.gov
References
Adams SM, Bornemann PH. Ulcerative colitis. Am Fam Physician. 2013;87(10):699-705. PMID: 23939448 pubmed.ncbi.nlm.nih.gov/23939448/.
Ananthakrishnan AN, Regueiro MD. Management of inflammatory bowel disease. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 116.
Bernstein CN, Fried M, Krabshuis JH, et al. World Gastroenterology Organization Practice Guidelines for the diagnosis and management of IBD in 2010. Inflamm Bowel Dis. 2010;16(1):112-124. PMID: 19653289 pubmed.ncbi.nlm.nih.gov/19653289/.
Bressler B, Marshall JK, Bernstein CN, et al. Clinical practice guidelines for the medical management of nonhospitalized ulcerative colitis: the Toronto consensus. Gastroenterology. 2015;148(5):1035-1058.e3. PMID: 25747596 pubmed.ncbi.nlm.nih.gov/25747596/.
Chang JT. Pathophysiology of inflammatory bowel diseases. N Engl J Med. 2020;383(27):2652-2664. PMID: 33382932 pubmed.ncbi.nlm.nih.gov/33382932/.
Farraye FA, Odze RD, Eaden J, et al. AGA medical position statement on the diagnosis and management of colorectal neoplasia in inflammatory bowel disease. Gastroenterology. 2010;138(2):738-745. PMID: 20141808 pubmed.ncbi.nlm.nih.gov/20141808/.
Feuerstein JD, Isaacs KL, Schneider Y, et al; AGA Institute Clinical Guidelines Committee. AGA Clinical Practice Guidelines on the management of moderate to severe ulcerative colitis. Gastroenterology. 2020;158(5):1450-1461. PMID: 31945371 pubmed.ncbi.nlm.nih.gov/31945371/.
Flynn S, Eisenstein S. Inflammatory bowel disease presentation and diagnosis. Surg Clin North Am. 2019;99(6):1051-1062. PMID: 31676047 pubmed.ncbi.nlm.nih.gov/31676047/.
Kaplan GG, Ng SC. Epidemiology, pathogenesis, and diagnosis of inflammatory bowel diseases. In: Feldman M, Friedman LS, Brandt LJ, eds. Sleisenger and Fordtran's Gastrointestinal and Liver Disease. 11th ed. Philadelphia, PA: Elsevier; 2021:chap 115.
Kelsen JR, Russo P, Sullivan KE. Early-onset inflammatory bowel disease. Immunol Allergy Clin North Am. 2019;39(1):63-79. PMID: 30466773 pubmed.ncbi.nlm.nih.gov/30466773/.
Ko CW, Singh S, Feuerstein JD, et al; American Gastroenterological Association Institute Clinical Guidelines Committee. AGA Clinical Practice Guidelines on the management of mild-to-moderate ulcerative colitis. Gastroenterology. 2019;156(3):748-764. PMID: 30576644 pubmed.ncbi.nlm.nih.gov/30576644/.
Lichtenstein GR. Inflammatory bowel disease. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier Saunders; 2020:chap 132.
Nguyen GC, Seow CH, Maxwell C, et al. The Toronto consensus statements for the management of inflammatory bowel disease in pregnancy. Gastroenterology. 2016;150(3):734-757.e1. PMID: 26688268 pubmed.ncbi.nlm.nih.gov/26688268/.
Rojas-Khalil Y, Galandiuk S. Management of chronic ulcerative colitis. In: Cameron JL, Cameron AM, eds. Current Surgical Therapy. 13th ed. Philadelphia, PA: Elsevier; 2020:173-180.
Rosen MJ, Dhawan A, Saeed SA. Inflammatory bowel disease in children and adolescents. JAMA Pediatr. 2015;169(11):1053-1060. PMID: 26414706 pubmed.ncbi.nlm.nih.gov/26414706/.
Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. ACG Clinical Guideline: ulcerative colitis in adults. Am J Gastroenterol. 2019;114(3):384-413. PMID: 30840605 pubmed.ncbi.nlm.nih.gov/30840605/.
Sherlock ME, MacDonald JK, Griffiths AM, Steinhart AH, Seow CH. Oral budesonide for induction of remission in ulcerative colitis. Cochrane Database Syst Rev. 2015;(10):CD007698. PMID: 26497719 pubmed.ncbi.nlm.nih.gov/26497719/.
Shouval DS, Rufo PA. The Role of environmental factors in the pathogenesis of inflammatory bowel diseases: a review. JAMA Pediatr. 2017;171(10):999-1005. PMID: 28846760 pubmed.ncbi.nlm.nih.gov/28846760/.
Stein RE, Baldassano RN. Inflammatory bowel disease. In: Kliegman RM, St. Geme JW, Blum NJ, Shah SS, Tasker RC, Wilson KM, eds. Nelson Textbook of Pediatrics. 21st ed. Philadelphia, PA: Elsevier; 2020:chap 362.
Timmer A, Patton PH, Chande N, McDonald JW, MacDonald JK. Azathioprine and 6-mercaptopurine for maintenance of remission in ulcerative colitis. Cochrane Database Syst Rev. 2016;(5):CD000478. PMID: 27192092 pubmed.ncbi.nlm.nih.gov/27192092/.
Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Ulcerative colitis. Lancet. 2017;389(10080):1756-1770. PMID: 27914657 pubmed.ncbi.nlm.nih.gov/27914657/.
Van Assche G, Lewis JD, Lichtenstein GR, et al. The London position statement of the World Congress of Gastroenterology on Biological Therapy for IBD with the European Crohn's and Colitis Organisation: safety. Am J Gastroenterol. 2011;106(9):1594-1602. PMID: 21844919 pubmed.ncbi.nlm.nih.gov/21844919/.
Review Date: 6/26/2021
Reviewed By: Michael M. Phillips, MD, Emeritus Professor of Medicine, The George Washington University School of Medicine, Washington, DC. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.