
Parkinson disease - InDepth
Paralysis agitans - InDepth; Shaking palsy - InDepthAn in-depth report on the causes, diagnosis, and treatment of Parkinson disease.
Highlights
What is Parkinson Disease?
Parkinson disease is a neurological disease that affects movement, muscle control, intellectual abilities, memory, and balance. Parkinson disease most commonly affects people ages 55 to 75 years, but it can also develop in younger people. The disease is progressive, with symptoms becoming more severe over time. Presently, Parkinson disease is incurable.
Symptoms of Parkinson Disease
Parkinson disease may be difficult to diagnose in its early stages. The disease is generally diagnosed on the basis of symptoms, which may include:
- Tremors (shaking) in the hands, arms, legs, and face
- Slowness of movement, especially when initiating motion
- Muscle rigidity
- Difficulty with walking, balance, and coordination
- Difficulty eating and swallowing
- Digestive problems
- Speech problems
- Depression and difficulties with memory and thought processes
Treatment
There is no cure for Parkinson disease. Treatments focus on controlling symptoms and improving quality of life.
- Lifestyle Changes. Good nutrition, regular exercise, and stress management can make living with Parkinson easier.
- Rehabilitation Therapy. Physical therapy is an important part of Parkinson treatment. Speech and occupational therapy are also helpful. Rehabilitation can help improve balance, mobility, speech, and functional abilities.
- Medications. Because Parkinson disease symptoms are due to a deficiency of the brain chemical dopamine, the main drug treatments help increase dopamine levels in the brain. Levodopa, usually combined with carbidopa, is the standard drug treatment. Other types of medication may also be used. Unfortunately, many of these drugs can cause side effects and lose effectiveness over time.
- Surgery. In some cases of advanced-stage Parkinson disease, surgery may help to control motor problems. Deep brain stimulation is currently the preferred surgical method.
Introduction
Parkinson disease (PD) is a slowly progressive neurological disease that affects movement, muscle control, mentation, memory, and balance. Parkinson disease is part of a group of conditions called motor system disorders, which are associated with the loss of dopamine-producing brain cells. The term "parkinsonism" refers to these dopamine-associated motor disorders, which include Parkinson disease. Collectively, all neurologic diseases which affect movements, either by slowing them down or causing extra movements, are known as "movement disorders". This group of diseases is usually treated and managed by neurologists.
Parkinson Disease and Dopamine Loss
Parkinson disease occurs from the following process in the brain:
- PD develops as cells are destroyed in certain parts of the brain stem, particularly the crescent-shaped cell mass known as the substantia nigra.
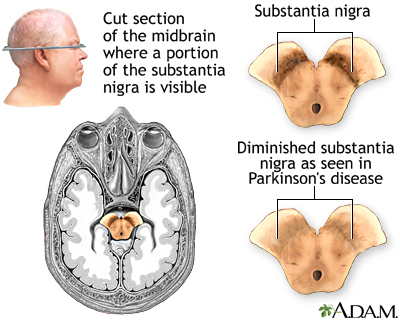
Parkinson disease is a slowly progressive disease that affects movement, muscle control, and balance.
- Nerve cells in the substantia nigra send out fibers to the corpus striatum, gray and white bands of tissue located in both sides of the brain.
- There the cells release dopamine, an essential neurotransmitter (chemical messenger in the brain). Loss of dopamine in the corpus striatum is the primary defect in Parkinson disease. The clinical features of Parkinson disease such as slowness of movement appear when up to 90% of dopaminergic neurons in the substantia nigra are destroyed.
- A key molecule causing Parkinson disease is a protein called alpha-synuclein, which forms toxic deposits that kill brain cells. These deposits are known as Lewy bodies. Parkinson disease is considered a synucleinopathy (a condition caused by alpha-synuclein). Another synucleinopathy is Lewy body dementia.
Loss of dopamine impairs the nerves and muscles controlling movement and coordination, resulting in the major symptoms of Parkinson disease. Dopamine also appears to be important for efficient information processing. Dopamine deficiencies may be responsible for the problems in memory and concentration that affect many people with Parkinson.
Causes
Doctors don't know what causes Parkinson disease. A combination of genetic and environmental factors likely plays a role.
Genetic FactorsSpecific genetic factors appear to play a strong role in early-onset Parkinson disease, an uncommon form of the disease. Multiple genetic factors may also be involved in some cases of late-onset Parkinson disease.
Environmental FactorsEnvironmental factors are probably not the sole cause of Parkinson disease, but they may trigger the condition in people who are genetically susceptible.
Some evidence implicates pesticides and herbicides as possible factors in some cases of Parkinson disease. A higher incidence of parkinsonism has long been observed in people who live in rural areas, particularly those who drink private well water or are agricultural workers.
Risk Factors
Age
The average age of onset of Parkinson disease is 55. About 10% of Parkinson cases are in people younger than age 40. Older adults are at higher risk for both parkinsonism and Parkinson disease.
Sex
Parkinson disease is more common in men than in women.
Genetics and Family History
People with siblings or parents who developed Parkinson at a younger age face an increased risk for the condition. However, relatives of patients who developed Parkinson at an older age appear to have an average risk. In rare cases of familial Parkinson disease, a single gene mutation is responsible for the condition. Genetic factors also play an important role in other patients, especially if their symptoms first occurred before age 50. Scientists have identified several gene changes that correlate with a higher risk for Parkinson disease, including mutations in the alpha-synuclein gene.
Race and Ethnicity
African Americans and Asian Americans appear to have a lower risk than Caucasians.
Possible Protective Factors
Both smoking and coffee drinking are associated with a lower risk for PD.
Smoking and NicotineCigarette smokers appear to have a lower risk for Parkinson disease, indicating possible protection by nicotine. This finding is, of course, no excuse to smoke. The few studies on nicotine replacement as a treatment for Parkinson have not provided any strong evidence that nicotine therapy provides benefits.
Coffee ConsumptionSome studies suggest that the risk for PD in coffee drinkers is lower than for non-coffee drinkers.
Complications
Parkinson disease (PD) is not fatal, but it can reduce longevity. The disease progresses more quickly in older people, and it may lead to severe incapacity within 10 to 20 years. Older people with PD also tend to have muscle freezing and greater declines in mental function and daily functioning than younger people. If PD starts without signs of tremor, it is likely to be more severe than if tremor is present. PD can severely interfere with patients' ability to move and can lead to falls and injuries from falls.
Parkinson disease can seriously impair the quality of life in any age group. In addition to motor symptoms (motion difficulties, tremors), Parkinson disease can cause various non-motor problems that have significant physical and emotional impacts on patients and their families. Loss of memory, impairment of judgment, decreased ability to think and reason, and eventually dementia are prominent non-motor abnormalities of PD.
Swallowing Problems
Swallowing problems (dysphagia) are sometimes associated with shorter survival time. Loss of muscle control in the throat not only impairs chewing and swallowing, which can lead to malnourishment, but also poses a risk for aspiration pneumonia. Swallowing problems can also interfere with adequate consumption of fiber and fluid, which can worsen constipation.
Emotional and Behavioral Problems
Depression is very common in people with Parkinson. The disease process itself causes changes in brain chemicals that affect mood and well-being. Anxiety is also very common and may present along with depression. Dementia is another serious problem which can happen in people with PD.
Some drug treatments, particularly dopamine agonists, can cause poor impulse control and compulsive behaviors, such as gambling, shopping, and increased sex drive. People who have pre-existing tendencies for novelty-seeking behavior, or a family or personal history of alcohol abuse, may be more likely to develop these problems. Deep brain stimulation (DBS) surgery may also increase the risk for compulsive gambling in people who have a history of gambling.
Cognitive and Memory Problems
Impaired Thinking (Cognitive Impairment)Defects in thinking, language, and problem solving skills may occur early on or later in the course of the disease. These problems can arise from the disease process or from the side effects of medications used to treat Parkinson. People with PD are slower in detecting associations, although (unlike in Alzheimer disease) once they discover them they are able to apply this knowledge to other concepts.
DementiaDementia occurs in about two-thirds of people with Parkinson, especially those who developed PD after age 60. Dementia is the significant loss of cognitive functions such as memory, judgment, attention, and abstract thinking. It is most likely to occur in older people who have had major depression. Having PD marked by muscle rigidity (akinesia) rather than tremor and early hallucinations also increases the risk for dementia. (Visual hallucinations can also occur as a side effect of dopamine medication.) Unlike Alzheimer disease, language is not usually affected in Parkinson-related dementia.
Sleep Disorders
Excessive daytime sleepiness, insomnia, and other sleep disorders are common in PD, both from the disease itself and the drugs that treat it. Bladder problems can also contribute to sleep disturbances. Many people with Parkinson disease also suffer from nighttime leg cramps and restless legs syndrome. Some of the medications used for PD may cause vivid dreams, as well as waking hallucinations. Acting out dreams, sometimes violently, can be a first sign of Parkinson, but can also develop and worsen as the disease progresses.
Sexual Dysfunction
Although Parkinson disease and its treatments can cause compulsive sexual behavior, the disease can also cause a loss of sexual desire in both men and women. For men, erectile dysfunction can be a complication of Parkinson.
Bowel and Bladder Complications
Constipation is a common complication of Parkinson disease. It is often caused by muscle weakness that can slow down the action of the digestive system. Weakness in pelvic floor muscles can also make it difficult to defecate. In addition, swallowing problems associated with muscle weakness may make it difficult to eat enough fiber-rich foods and drink enough fluids, which can also cause constipation. Constipation may also occur as a side effect of some Parkinson medications.
People with Parkinson disease may experience urinary incontinence, including increased urge and frequency, although this is less common than constipation. PD can also cause urinary retention (incomplete emptying of the bladder).
Orthostatic Hypotension (Low Blood Pressure)
Orthostatic hypotension is a rapid drop in blood pressure (hypotension is the medical term for low blood pressure) triggered by a sudden change in body position. It usually occurs when standing up after sitting or lying down.
Parkinson disease, and the medications used to treat it, can also cause orthostatic hypotension. Lifestyle factors that can contribute to orthostatic hypotension include dehydration, alcohol, hot drinks and foods, and overexertion.
Symptoms of orthostatic hypotension include dizziness, lightheadedness, weakness, blurred vision, loss of balance, and fainting. Orthostatic hypotension can increase the risk for falls and injuries, and limit patients' ability to perform daily tasks that require standing or walking.
Sensory Problems
Decreased Sense of SmellMany people with PD experience an impaired sense of smell. Often they may also experience a decreased sense of taste.
Vision ProblemsVision may be affected, including impaired color perception and contrast sensitivity.
PainPainful symptoms associated with Parkinson disease include back pain, neck pain, tingling, and aching. Pain in Parkinson often results from dystonia (involuntary muscle contractions and spasms that can cause twisting and jerking), as well as from the gastrointestinal system.
Skin Problems
People with PD often develop skin problems, including excessively oily, dry, or flaking skin. Of greatest concern, Parkinson disease appears to be associated with a higher risk for developing melanoma (an aggressive skin cancer). People with Parkinson disease should have regular screenings with a dermatologist to check for skin changes that may indicate melanoma.
Falls
People with PD are prone to falls and each fall in its own place can cause serious or even fatal injuries.
Symptoms
Tremors
Parkinson disease (PD) symptoms often start with tremor, which may occur in the following ways:
- Tremors may be only occasional at first, starting in one finger and spreading over time to involve the whole arm. The tremor is often rhythmic, 4 to 5 cycles per second, and frequently causes an action of the thumb and fingers known as pill rolling.
- Tremors can occur when the limb is at rest or when it is held up in a stiff unsupported position. They usually disappear briefly during movement and do not occur during sleep.
- Tremors can also eventually occur in the head, lips, tongue, and feet. Symptoms can occur on one or both sides of the body.
About 25% of people with PD do not develop tremor.
Motion and Motor Impairment
Many PD symptoms involve motor impairment caused by problems in the brain nerves that regulate movement:
- Slowness of motion, particularly when initiating any movement (a condition called akinesia or bradykinesia), is one of the classic symptoms of Parkinson disease.
- A stooped posture and a slow, shuffling walk may eventually develop. The gait can be erratic and unsteady. After several years, muscles may freeze up or stall, usually when a person is making a turn or passing through narrow spaces, such as a doorway. Posture can be unstable and contribute to an increased risk for falls.
- Intestinal motility (the ability to swallow, digest, and eliminate) may slow down, causing eating problems and constipation.
- Muscles may become rigid. This symptom often begins in the legs and neck. Muscle rigidity in the face can produce a mask-like, staring appearance.
- Motor abnormalities that limit action in the hand may develop in late stages. Handwriting, for instance, often becomes small.
- Normally spontaneous muscle movements, such as blinking, may need to be done consciously.
- Speech problems, including soft voice or slurred speech, are common.
Other Symptoms of Parkinson Disease
Parkinson disease also causes non-motor symptoms, including fatigue, sleep problems, gastrointestinal and urinary disorders, sexual dysfunction, decreased sense of smell, and depression and anxiety. [See Complications section of this report.]Sialorrhea (drooling) is a common and bothersome symptom for those with Parkinson disease. It can cause chapped lips and skin around the mouth, dehydration, an unpleasant odor, and social embarrassment.
Diagnosis
Parkinson disease (PD) can be difficult to diagnose in its early stages. Doctors base their diagnosis on the person's medical history and symptoms evaluated during a neurological exam.
Brain scans such as computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET) may be used to rule out other neurological disorders. Genetic tests may be used to identify inherited forms of PD.
Medical History
A medical and personal history should include any relevant symptoms, as well as any medications taken, and information on other conditions the person may have.
Neurological Exam
In a neurological exam, the doctor will ask you to sit, stand, walk, and extend your arms. The doctor will observe your balance and coordination. PD may be suspected in people who have at least 2 of the following 4 symptoms, especially if they are more obvious on one side of the body:
- Tremor (shaking) when the limb is at rest
- Slowness of movement (bradykinesia)
- Rigidity, stiffness, or increased resistance to movement in the limbs or torso
- Poor balance (postural instability)
Drug Challenge Test
A levodopa challenge test may confirm a diagnosis of Parkinson disease. If your symptoms improve when you take the drug levodopa, you likely have Parkinson, and not another type of neurological disease.
Tests for Depression and Dementia
The American Academy of Neurology (AAN) recommends the Beck Depression Inventory or the Hamilton Depression Rating Scale to screen for depression in patients with Parkinson disease. The AAN recommends the Mini Mental State Examination (MMSE) and Cambridge Cognitive Examination (CAMCOG) tests to screen for dementia. During these tests, the patient answers a series of questions.
Ruling out Conditions that Mimic Parkinson Disease
Parkinsonism Plus SyndromesParkinson disease is the most common type of parkinsonism. Parkinsonism refers to a group of movement disorders that share similar symptoms with Parkinson disease, but also have unique symptoms of their own. About 15% of parkinsonism cases are due to conditions called Parkinson plus syndromes (PPS) or atypical parkinsonism. These syndromes include:
- Corticobasal degeneration. This condition is marked by apraxia (inability to perform coordinated movements or use familiar objects), stiffness that is more severe than typical Parkinson disease, and twitching or jerking in the hand.
- Lewy body dementia. One of the most common types of progressive dementia, symptoms include visual hallucinations and loss of spontaneous movement.
- Multiple system atrophy. Symptoms include fainting, constipation, erectile dysfunction, urinary retention, and loss of muscle coordination.
- Progressive supranuclear palsy. Marked by frequent falls, personality changes, and difficulty moving the eyes to focus on objects.
People with PPS often have earlier and more severe dementia than those with Parkinson disease. In addition, they do not usually respond to medications that are used to treat Parkinson disease.
Other Neurologic ConditionsMany medical conditions may cause some symptoms of Parkinson disease and parkinsonism. Hardening of the arteries (arteriosclerosis) in the brain can cause multiple small strokes, which can produce loss of motor control. Alzheimer disease can share similar symptoms with Parkinson and the conditions can exist together.
MedicationsSeveral drugs, including antipsychotic and antiseizure medications, can cause Parkinson-type symptoms.
Treatment
There is no cure for Parkinson disease (PD), but drugs, physical therapy, lifestyle changes, and surgical interventions can help control symptoms and improve quality of life.
Treatment for Parkinson Disease
Treatment for this complicated condition must be individualized. People with PD must work closely with their health care team throughout the course of the disease to tailor a treatment program to their particular and changing needs. No treatment method, including drug therapy, has been proven to change the course of the disease or slow disease progression. But many treatments can help ease symptoms and restore normal functioning for long periods of time.
Drug Therapy
The decision to start drug therapy usually arises when motor symptoms (movement problems, muscle rigidity, tremors) begin to interfere with daily functioning. The main types of drugs for treating Parkinson disease are:
- Levodopa/carbidopa
- Dopamine agonists
- MAO-B inhibitors
- Anticholinergics
- Amantadine
All of these drugs have side effects. Your health care provider will discuss with you the risks and benefits of various drugs, and will take into consideration such factors as your overall health, age, symptoms, stage of Parkinson disease, and other medical conditions you may have.
In general, levodopa/carbidopa is the standard drug for treating PD throughout its disease course, but other drugs may be used for its earlier stages. When levodopa is used for many years, it can "wear off" and symptom improvement ("on" time) may decrease while symptom worsening ("off" time) increases. Motor symptoms may also fluctuate unpredictably. Your health care provider may adjust the dosage or add another drug to your regimen to help boost levodopa's effectiveness.
Treatment for Advanced Parkinson Disease
For people with advanced Parkinson disease whose symptoms can no longer be controlled by medication, surgical treatment with deep brain stimulation may be an option. (Some recent research suggests this treatment may also be helpful for patients in earlier stages of the disease). Home modifications (wheelchair ramps, grab bars, and handrails) can help improve functional abilities and independent living. Treatment goals for all stages of Parkinson disease should focus on providing safety, comfort, and quality of life.
Treatments for Other Symptoms of Parkinson Disease
Conditions associated with non-motor impairment symptoms of Parkinson disease may need a variety of treatments.
DepressionMedications for PD-associated depression include older drugs such as the tricyclic antidepressant amitriptyline, as well as newer antidepressants, including selective serotonin reuptake inhibitors (SSRIs) and serotonin norepinephrine reuptake inhibitors (SNRIs) such as fluoxetine (Prozac, generic), sertraline (Zoloft, generic), paroxetine (Paxil, generic), and venlafaxine (Effexor, generic). The dopamine agonist pramipexole (Mirapex, generic) may also be helpful for Parkinson depression. Health care providers need to monitor antidepressants to make sure they do not worsen motor symptoms.
Psychotic Side EffectsPsychosis in Parkinson disease is often a side effect of medication. Doctors first try to adjust the dose of PD medications to see if psychotic side effects decrease without motor symptoms increasing. In some cases, doctors may prescribe an antipsychotic drug, usually quetiapine (Seroquel, generic). The antipsychotic clozapine (Clozaril, generic) is also effective, but it can have a serious side effect of lowering white blood cell count. Certain types of antipsychotic medications, such as olanzapine (Zyprexa, generic) and risperidone (Risperdal, generic), should not be used in people with PD because they can worsen Parkinson symptoms.
DementiaThe cholinesterase inhibitor drugs donepezil (Aricept, generic) and rivastigmine (Exelon, generic) are used to treat Alzheimer disease and are sometimes used for Parkinson. (Rivastigmine is FDA-approved for treatment of Parkinson dementia.) These drugs typically have at best a very modest benefit on cognitive function.
Daytime Sleepiness and FatigueModafinil (Provigil, generic), a drug used to treat narcolepsy, may be helpful for PD-associated sleepiness. Methylphenidate (Ritalin, generic) may be considered for treating fatigue.
Erectile DysfunctionPDE5 inhibitor drugs such as sildenafil (Viagra), tadalafil (Cialis), vardenafil (Levitra), and avanafil (Stendra) can be helpful for men with Parkinson disease who suffer from erectile dysfunction. However, these drugs may worsen orthostatic hypotension.
Orthostatic HypotensionOrthostatic hypotension is a sudden drop in blood pressure that occurs when rising from a sitting or lying down position. It causes dizziness and light-headedness. Lifestyle treatments include avoiding dehydration, carbohydrate-heavy meals, overexposure to heat, and vigorous exercise. Droxidopa (Northdera) is a new drug approved to treat orthostatic hypotension associated with Parkinson disease and other nervous system disorders. Droxidopa and similar medications have a risk of increasing blood pressure when lying down. People who take this drug must be sure to sleep with their head and upper body elevated.
ConstipationDietary changes should be the first step for addressing constipation. It is important to increase overall fiber and fluid consumption, but this can be difficult for people who have swallowing problems. Taking a stool softener such as docusate (Colace, generic) on a daily basis may help with bowel movements.
For people who need laxatives, bulk-forming fiber laxatives are considered the safest and are not habit-forming. They include psyllium (Metamucil, other brands, generic) and wheat dextrin (Benefiber, generic). Stimulant laxatives should be avoided as they can worsen bowel problems if used on a long-term basis. Check with your health care provider for advice about using other types of laxatives, suppositories, and enemas. Regular exercise is also helpful for constipation.
Drooling (sialorrhea)Glycopyrrolate, scopolamine, and injections of botulinum toxin may be used to relieve drooling symptoms.
Medications
Levodopa/Carbidopa
Levodopa, also called L-dopa, which is converted to dopamine in the brain, remains the gold standard for treating Parkinson disease (PD) symptoms. The standard preparations (Sinemet, Parcopa) combine levodopa with carbidopa, which improves the action of levodopa and reduces some of its side effects, particularly nausea. Sinemet is swallowed as a pill. Parcopa is a tablet that dissolves under the tongue.
Dosages vary, although the preparation is usually taken in 3 or 4 divided doses per day. This medication works best on an empty stomach, but some people find this causes nausea and prefer to take it with a light meal or snack. If you are taking levodopa/carbidopa along with food, it is important to avoid high-protein foods as they can interfere with drug absorption.
Levodopa/carbidopa helps improve mobility for many people with PD. It works best for treating difficulties with movement (akinesia) and muscle stiffness. It may be less effective for treating tremor, balance, coordination, and posture.
Levodopa/carbidopa does not prevent Parkinson disease progression. Over time, the dose of the drug has to be increased to be effective.
Side EffectsMany side effects of levodopa/carbidopa can be minimized by adjusting dosage. The most common side effects include nausea, vomiting, loss of appetite, low blood pressure, dizziness, and confusion.
Serious side effects include:
- Dyskinesia refers to involuntary muscle movements. Dyskinesia can take many forms, most often uncontrolled flailing of the arms and legs or chorea, rapid and repetitive motions that can affect the limbs, face, tongue, mouth, and neck. Dyskinesia may develop after long-term use of levodopa.
- Serious psychiatric side effects include agitation, hallucinations, delusions, and psychosis.
After several years of taking levodopa, many people with PD find that the drug's helpful effects last for shorter periods of time and that symptoms return before the next dose is due to be taken. When the medication wears off in between doses, symptoms may suddenly worsen ("off-time"). At other times of the day, symptoms may be well-controlled ("on-time"). Wearing off can develop gradually during the day, or it can occur intermittently and unpredictably.
An increase in dyskinesia (involuntary movements) and other motor symptoms (muscle stiffness, rigidity, slowness, cramping) are most commonly associated with the wearing-off effect. Some people may also experience non-motor symptoms, such as difficulty concentrating, anxiety, insomnia, fatigue, sweating, and trouble breathing. If symptoms improve when the next dose of levodopa/carbidopa is taken, this is a clear sign of the wearing-off effect.
There are different approaches for managing wearing off and off-time. Your doctor may recommend:
- Using a controlled-release formulation of levodopa/carbidopa (Sinemet CR, Rytary), which slowly releases the drug into your bloodstream throughout the day.
- Switching to Stalevo, a levodopa/carbidopa drug that also includes the COMT inhibitor entacapone.
- Using apomorphine hydrochloride (Apokyn) to improve movements during off episodes.
- Adding another drug such as a COMT inhibitor, MAO-B inhibitor, or dopamine agonist to your current medication regimen.
- A new form of inhalation powder levodopa (Inbrija) has been FDA-approved for "off-time" episodes in patients currently treated with levodopa/carbidopa.
Making some adjustments to your food schedule may also help with wearing off. Try to take levodopa/carbidopa on an empty stomach, at least 30 minutes before eating. High-protein foods can especially interfere with levodopa absorption.
Dopamine Agonists
Levodopa is converted into dopamine in the brain. In contrast, dopamine agonists mimic the action of dopamine by stimulating dopamine receptors in the brain. A dopamine agonist drug may be used as an initial medication in the early stages of PD to delay the need for levodopa, or it may be used along with levodopa/carbidopa in later stages of the disease.
When used alone, these drugs are less likely to cause dyskinesia than levodopa, but they may be less effective than levodopa for controlling motor symptoms. There is debate about the value of dopamine agonists as first-line therapy for Parkinson disease. Some research suggests that early treatment with dopamine agonists may not provide any long-term advantages compared with starting treatment with levodopa/carbidopa.
BrandsPramipexole (Mirapex, generic) and ropinirole (Requip, generic) are the most commonly prescribed oral dopamine agonists. Rotigotine (Neupro) is a skin patch that is applied once a day. Apomorphine (Apokyn) is a self-injectable dopamine agonist that is used as a rescue medication for quickly treating off-time motor symptoms in advanced PD.
Side EffectsCommon side effects of dopamine agonists include nausea, confusion, and leg swelling. More serious concerns include:
- Orthostatic hypotension (sudden drop in blood pressure upon standing up).
- Nightmares, hallucinations, and psychosis -- especially for people with advanced disease.
- Excessive sleepiness and sudden sleep attacks. Be aware of this side effect, particularly if you drive.
- Compulsive behaviors that are associated with a loss of impulse control, including compulsive gambling, sexual behavior, shopping, and eating.
- Heart failure may be a possible concern. To date, the FDA is not able to determine whether pramipexole increases the risk of heart failure.
Monoamine Oxidase B (MAO-B) Inhibitors
MAO-B inhibitor drugs block monoamine oxidase B (MAO-B), an enzyme that inactivates dopamine. Selegiline (Eldepryl, Zelapar) and rasagiline (Azilect) are MAO-B inhibitors used for treating Parkinson disease.
These drugs may be used alone in the early stages of PD to treat mild symptoms (such as tremor) and delay the need for levodopa. They may also be used in combination with levodopa in later stages to enhance the effects of levodopa and help manage motor fluctuations. Rasagiline may also be used in combination with dopamine agonists. Many people with PD notice only small benefits in improvement with these drugs.
Side EffectsCommon side effects of MAO-B inhibitors include flu symptoms, dizziness, and insomnia. More serious side effects may include agitation, confusion, and hallucination.
Talk with your health care provider about any other medications (both prescription and over-the-counter) and supplements you are taking. MAO-B inhibitors can interact with a number of medications, including narcotics, pain relievers, cough suppressants, and antidepressants (including the herbal remedy St. John's wort). Foods high in the amino acid tyramine may cause a dangerous increase in blood pressure, particularly if you are taking a high dose of this medicine. Foods to be avoided include processed lunch meats, soy sauce, aged cheeses, and beer.
Catechol-O-Methyl Transferase (COMT) Inhibitors
Catechol-O-methyl transferase (COMT) inhibitor drugs are used along with levodopa/carbidopa to increase and prolong levodopa's effectiveness and prevent wearing off. Entacapone (Comtan, generic) is the standard COMT inhibitor. Stalevo (generic) is a pill that combines entacapone, levodopa, and carbidopa. A third COMT inhibitor, tolcapone (Tasmar), is only rarely prescribed due to its risks for liver damage.
Side EffectsCOMT inhibitors are always used in combination with levodopa/carbidopa and may increase levodopa's dyskinesia side effects. Other side effects may include low blood pressure when standing up (orthostatic hypotension), nausea, dizziness, diarrhea, and urine discoloration.
Anticholinergic Drugs
Anticholinergics were the first drugs used for PD, but they have largely been replaced by dopamine drugs. They are generally used only to control tremor in the early stages. Among the many anticholinergics are trihexyphenidyl (Artane, Trihexane, generic) and benztropine (Cogentin, generic).
Side EffectsAnticholinergics commonly cause dryness of the mouth (which can actually be an advantage in some people who experience drooling). Other side effects are nausea, urinary retention, blurred vision, and constipation. These drugs can increase heart rate and worsen constipation. Anticholinergics can sometimes cause significant mental problems, including memory loss, confusion, and even hallucinations. People with glaucoma should use these drugs with caution.
Amantadine
Amantadine (generic) stimulates the release of dopamine and may be used to provide temporary relief of early mild symptoms such a tremor and rigidity. It is sometimes prescribed along with levodopa/carbidopa for advanced PD to help control motor fluctuations and dyskinesia.
Side EffectsSide effects are similar to those of anticholinergic drugs, and may include swollen ankles and, in rare cases, mottled skin. Amantadine can also cause visual hallucinations, confusion, and memory loss.
Surgery
Surgical procedures are recommended for specific individuals with advanced Parkinson disease (PD) whose symptoms are not controlled by drug treatments. Surgical treatment cannot cure Parkinson disease, but it may help control symptoms such as motor fluctuations and dyskinesia.
Deep brain stimulation is the current standard surgical approach for Parkinson disease. It has largely replaced pallidotomy and thalamotomy, older operations that destroy tissue in certain parts of the brain, which are rarely performed anymore.
Deep Brain Stimulation
In deep brain stimulation (DBS), also called neurostimulation, an electric pulse generator controls symptoms such as severe tremors, wearing-off fluctuations, and dyskinesia. The generator is similar to a heart pacemaker. It sends electrical pulses to specific regions of the brain. Candidates most likely to benefit from DBS are those who have advanced PD, have responded well to levodopa drug treatment, are younger in age, and do not have significant cognitive or psychiatric problems. Some recent research suggests that DBS may also benefit people in earlier stages of the disease who have early signs of motor symptoms.
For treatment of motor symptoms, DBS usually targets one of two areas of the brain: the subthalamic nucleus (STN) or the globus pallidus pars interna (GPi). Research indicates that both areas are equally likely to respond well to DBS. DBS targeting the STN may allow people to use less medication, but treatment of this brain area may worsen depression, apathy, impulsivity, ease of using words, and falls.
For treatment of disabling tremors, DBS may be used to target the STN, GPi, or the ventral intermediate nucleus of the thalamus.
DBS should be performed by an experienced neurosurgeon who is trained in stereotactic neurosurgery (surgery that uses 3-dimensional imaging to help target specific areas of the brain).
The procedure is performed as follows:
- Before the procedure, the neurosurgeon uses magnetic resonance imaging (MRI), computed tomography (CT), or other types of imaging techniques to pinpoint the exact areas of the brain where the DBS electrodes will be inserted.
- The neurosurgeon implants a tiny pulse generator near the collarbone, which is connected to 4 electrodes that have been implanted in the target area in the brain.
- The generator delivers programmed pulses to this area, which the patient can turn on and off using a magnet held over the skin. When on, the pulses suppress symptoms.
- The most common complication is infection at the surgical site.
The benefits of DBS appear to be long lasting, but it may take 3 to 6 months to achieve results. During this time, doctors may need to adjust the implanted device. Researchers are still trying to determine the best surgical techniques for implanting the DBS device, and how to best select the people who are most likely to benefit.
Pallidotomy and Thalamotomy
Pallidotomy and thalamotomy are surgical procedures that destroy brain tissue in regions of the brain associated with Parkinson symptoms such as dyskinesia, rigidity, and tremor. In these procedures, a surgeon drills a small hole in the patient's skull and inserts an electrode to destroy brain tissue. Pallidotomy targets the global pallidus area. Thalamotomy targets the thalamus. Because these procedures permanently eliminate brain tissue, most doctors now recommend deep brain stimulation instead of pallidotomy or thalamotomy.
Surgical complications may include behavioral or personality changes, trouble speaking and swallowing, facial paralysis, and vision problems. Weight gain after surgery is also common.
A new method for thalamotomy using focused ultrasound is under investigation for people with tremor-dominant PD who are not responding to medication.
Stem Cell Implantation
Scientists are investigating whether stem cells may eventually help treat Parkinson disease. Experimental surgery has shown promise using fetal brain cells rich in dopamine implanted in the substantia nigra area of the brain. Because the use of embryonic stem cells is controversial, researchers are studying alternative types of cells, including stem cells from adult brains and cells from human placentas or umbilical cords. All of this research is still preliminary.
Lifestyle Changes
Nutrition
No special diets or foods can slow the progression of Parkinson disease (PD), but certain dietary strategies may help manage symptoms.
ProteinIf you are on levodopa, high levels of protein in your diet can affect the absorption of some medications and can reduce the drug's effectiveness. Avoiding protein altogether is not the solution, since malnutrition can result. Most health care providers recommend reducing protein or eating most of your protein at the evening meal. Discuss a low-protein diet and other nutritional strategies with your health team.
Good control of protein intake may help minimize fluctuations and wearing-off, and allow some people with PD to reduce their daily levodopa dosage.
Fruits, Vegetables, and FiberEating whole grains, fresh fruits, and vegetables is the best approach for any healthy life. A diet rich in fruits and vegetables may help protect nerve cell function. Many of these foods are also rich in fiber, which is particularly important for helping to prevent constipation.
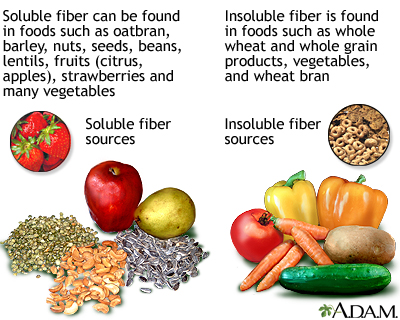
Dietary fiber is the part of food that is not affected by the digestive process in the body. Only a small amount of fiber is metabolized in the stomach and intestine. The rest is passed through the gastrointestinal tract and makes up part of the stool. There are two types of dietary fiber, soluble and insoluble. Soluble fiber retains water and turns to gel during digestion. It also slows digestion and nutrient absorption from the stomach and intestine. Soluble fiber is found in foods such as oat bran, barley, nuts, seeds, beans, lentils, peas, and some fruits and vegetables. Insoluble fiber appears to speed the passage of foods through the stomach and intestines and adds bulk to the stool. It is found in foods such as wheat bran, vegetables, and whole grains. One of the best sources of fiber comes from legumes, the group of foods containing dried peas and beans.
If you are used to eating a low-fiber diet, you should try to gradually increase the amount of fiber. It is best to obtain dietary fiber, soluble or insoluble, in the natural form of whole grains, nuts, legumes, fruits, and vegetables. If it proves difficult to do so, psyllium (found in products such as Metamucil) is an excellent soluble fiber supplement. Drinking lots of fluids is particularly important for preventing constipation.
Weight LossFor reasons that are not completely understood, many people with PD experience weight loss. Parkinson disease can affect a person's sense of smell and taste, which may make food less appetizing. Tremors (shaking) and swallowing problems can make it more difficult and tiring to eat. If you find that you are losing weight without trying, talk with your health care provider or dietitian about developing a diet plan that will meet your caloric needs.
Herbs and SupplementsThere is currently no evidence for the effectiveness of any herb or dietary supplement in the treatment of Parkinson disease. Coenzyme Q10 is the most-studied supplement for early-stage PD. Clinical trials have failed to show it has any benefits.
Ginger is one natural remedy that has well-established properties for easing nausea. A simple tea made from boiling ginger root may help alleviate nausea symptoms associated with many Parkinson disease medications.
Let your health care provider know about any herb or dietary supplement you are taking, or considering taking. Some products, such as St. John's wort, can interact and interfere with the effectiveness of Parkinson medications.
Exercise
Regular exercise is important for people in all stages of Parkinson disease. Exercise has a wide range of benefits. It can improve muscle strength and agility, which helps promote better walking and balance. Exercise can also help control symptoms such as fatigue, constipation, and depression.
Types of ExerciseHealth care providers recommend that people with PD incorporate stretching, resistance, and aerobic exercise into their routine. Some suggestions include:
- In the gym, walking on a treadmill, even at low intensity, can help improve walking gait and speed as well as cardiovascular fitness. Cycling on a stationary bike is also good aerobic exercise.
- Stretching and resistance exercise is the best way to build muscle strength. Weight training is a type of resistance exercise.
- Tai chi, a Chinese martial art that emphasizes slow flowing motions and gentle movements, may help people with mild-to-moderate Parkinson improve strength and balance and reduce the risk of falls. Yoga is also an excellent and gentle exercise for stretching, strengthening, and relaxation.
- Music helps people with PD move more smoothly and easily. Dance is an excellent way to increase flexibility and endurance.
- For people with more advanced Parkinson, certain exercise techniques can help manage rigidity and gait issues. It's a good idea to continually make efforts to practice movement, even simple ones, such as marching in place, making circular arm movements, and raising the legs up and down while sitting.
Try to practice regular daily activities that simplify actions and reduce the incidence of muscle freezing. Most often, freezing occurs when a person with PD begins to move or is presented with an obstacle. The following tips may be helpful:
- Rock from side to side.
- If the legs feel frozen, lift the toes. This simple action may free the spasm in some cases.
- Hum marching tunes. Music helps people with PD move and get out of bed in the morning.
- Divide actions into separate components, which may prevent the freezing that occurs from trying to coordinate too many physical operations at one time. For instance, when going through a doorway, approach the door, stop at the door, open it, stop, and then walk through the doorway.
- Simply being touched by another person can sometimes release muscle freezing (although people with PD should never be pulled or pushed).
Practicing new methods for standing, walking, and turning may help retain balance and reduce the risk of falls. The following tips may be helpful:
- Take large steps when walking forward, raising the toes at the forward step, and hitting the ground with the heel.
- Take small steps while turning.
- When walking or turning, keep the legs 12 to 15 inches apart to provide a wide base.
- Do not wear rubber- or crepe-soled shoes because they grip the floor and may cause you to fall forward.
- Using devices that keep a rhythmic beat, such a metronome (a simple device used by musicians to keep time), may help you walk faster and take longer steps.
Rehabilitation Therapies
People with PD can benefit from working with rehabilitative therapists. They include physical therapy, occupational therapy, and speech therapy. Art therapies (including dance therapy and music therapy) may also be helpful.
Physical TherapyExercise is an important component of rehabilitation. Physical therapy can help with physical function and quality of life. It usually includes active and passive exercise, gait training, and practice in normal activities. A physical therapist can help with passive exercise, stretching and manipulating muscles to help prevent deterioration and shortening. Active exercises are used to help range-of-motion, coordination, and speed. A physical therapist can also advise on how to best use mobility aids (such as canes, crutches, and scooters) and other assistive devices.
Speech TherapySpeech therapy may help those who develop a monotone voice and lose volume. Certain techniques, such as the Lee Silverman Voice Technique, are designed specifically to help people with Parkinson disease speak louder. A speech therapist can also help evaluate and monitor swallowing issues.
Occupational TherapyOccupational therapists help people learn how to improve their functioning and independence within their home and workplace environments. They can help people better manage activities of daily living, including bathing, dressing, and grooming. Occupational therapists can provide professional advice on what sort of adaptive tools, such as grab bars, should be used in the bathroom, bedroom, and kitchen. They can advise on mobility devices such as wheelchairs and scooters.
Stress Management
Relaxation techniques and staying mentally active are important for managing stress and dealing with feelings of depression and anxiety:
- Stress management includes deep breathing and other relaxation techniques, meditation, biofeedback, music therapy, yoga, tai chi, and massage therapy. Exercise is also an excellent way to reduce stress and can be incorporated into activities such as gardening and golf.
- Find new hobbies. People with PD may find that symptoms interfere with activities they once enjoyed. Developing new hobbies can help you stay positive and keep you mentally alert.
- Caregivers need to evaluate and manage their own stress and fatigue levels. There are many support organizations and resources available to help caregivers deal with the challenges of caring for a loved one with Parkinson disease.
- Psychological counseling is also appropriate.
Resources
National Institute of Neurological Disorders and Stroke -- www.ninds.nih.gov
American Academy of Neurology -- www.aan.com
American Parkinson Disease Association -- www.apdaparkinson.org
The Michael J. Fox Foundation for Parkinson's Research -- www.michaeljfox.org
References
Armstrong MJ, Okun MS. Diagnosis and treatment of Parkinson disease: a review. JAMA. 2020;323(6):548-560. PMID: 32044947 pubmed.ncbi.nlm.nih.gov/32044947/.
Ascherio A, Schwarzschild MA. The epidemiology of Parkinson's disease: risk factors and prevention. Lancet Neurol. 2016;15(12):1257-1272. PMID: 27751556 pubmed.ncbi.nlm.nih.gov/27751556/.
Balestrino R, Schapira AHV. Parkinson disease. Eur J Neurol. 2020;27(1):27-42. PMID: 31631455 pubmed.ncbi.nlm.nih.gov/31631455/.
Bond AE, Shah BB, Huss DS, et al. Safety and efficacy of focused ultrasound thalamotomy for patients with medication-refractory, tremor-dominant Parkinson disease: a randomized clinical trial. JAMA Neurol. 2017;74(12):1412-1418. PMID: 29084313 pubmed.ncbi.nlm.nih.gov/29084313/.
Del Rey NL, Quiroga-Varela A, Garbayo E, et al. Advances in Parkinson's disease: 200 years later. Front Neuroanat. 2018;12:113. PMID: 30618654 pubmed.ncbi.nlm.nih.gov/30618654/.
Elbers RG, Verhoef J, van Wegen EE, Berendse HW, Kwakkel G. Interventions for fatigue in Parkinson's disease. Cochrane Database Syst Rev. 2015;(10):CD010925. PMID: 26447539 pubmed.ncbi.nlm.nih.gov/26447539/.
Fox SH, Katzenschlager R, Lim SY, et al; Movement Disorder Society Evidence-Based Medicine Committee. International Parkinson and Movement Disorder Society evidence-based medicine review: Update on treatments for the motor symptoms of Parkinson's disease. Mov Disord. 2018;33(8):1248-1266. PMID: 29570866 pubmed.ncbi.nlm.nih.gov/29570866/.
Haq IU, Tate JA, Siddiqui MS, Okun MS. Clinical overview of movement disorders. In: Winn HR, ed. Youmans and Winn Neurological Surgery. 7th ed. Philadelphia, PA: Elsevier; 2017:chap 84.
Jankovic J. Parkinson disease and other movement disorders. In: Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 96.
Jankovic J, Lang AE. Diagnosis and assessment of Parkinson disease and other movement disorders. In: Jankovic J, Mazziotta JC, Pomeroy SL, Newman NJ, eds. Bradley and Daroff's Neurology in Clinical Practice. 8th ed. Philadelphia, PA: Elsevier; 2022:chap 24.
Jellinger KA. Neuropathology of movement disorders. In: Winn HR, ed. Youmans and Winn Neurological Surgery. 7th ed. Philadelphia, PA: Elsevier; 2017:chap 83.
Kalia LV, Lang AE. Parkinson's disease. Lancet. 2015;386(9996):896-912. PMID: 25904081 pubmed.ncbi.nlm.nih.gov/25904081/.
Mirelman A, Bonato P, Camicioli R, Ellis TD, Giladi N, Hamilton JL, Hass CJ, Hausdorff JM, Pelosin E, Almeida QJ. Gait impairments in Parkinson's disease. Lancet Neurol. 2019;18(7):697-708. PMID: 30975519 pubmed.ncbi.nlm.nih.gov/30975519/.
Mitchell KT, Ostrem JL. Surgical treatment of Parkinson disease. Neurol Clin. 2020;38(2):293-307. PMID: 32279711 pubmed.ncbi.nlm.nih.gov/32279711/.
Okun MS, Lang AE. Parkinsonism. In: Goldman L, Schafer AI, eds. Goldman-Cecil Medicine. 26th ed. Philadelphia, PA: Elsevier Saunders; 2020:chap 381.
Parnetti L, Gaetani L, Eusebi P, Paciotti S, Hansson O, El-Agnaf O, Mollenhauer B, Blennow K, Calabresi P. CSF and blood biomarkers for Parkinson's disease. Lancet Neurol. 2019;18(6):573-586. PMID: 30981640 pubmed.ncbi.nlm.nih.gov/30981640/.
Radder DLM, Sturkenboom IH, van Nimwegen M, et al. Physical therapy and occupational therapy in Parkinson's disease. Int J Neurosci. 2017;127(10):930-943. PMID: 28007002 pubmed.ncbi.nlm.nih.gov/28007002/.
US Food and Drug Administration website. FDA Drug Safety Communication: Ongoing safety review of Parkinson’s drug Mirapex (pramipexole) and possible risk of heart failure. www.fda.gov/drugs/drug-safety-and-availability/fda-drug-safety-communication-ongoing-safety-review-parkinsons-drug-mirapex-pramipexole-and-possible. Updated on 01/19/2016. Accessed on 05/31/2021.
Review Date: 5/31/2021
Reviewed By: Joseph V. Campellone, MD, Department of Neurology, Cooper Medical School at Rowan University, Camden, NJ. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.