
Vasectomy and vasectomy reversal - InDepth
Male sterilization - InDepth; Vasovasostomy - InDepth; Vasoepididymostomy - InDepth; Sterilization surgery - male - InDepth; No-scalpel vasectomy - InDepth; NSV - InDepth; Family planning - vasectomy - InDepth; Contraception - vasectomy - InDepthAn in-depth report on vasectomy as a method of male birth control and reversal surgeries.
Highlights
Vasectomy
Vasectomy is a safe and effective surgical operation for male sterilization, a permanent form of birth control. Vasectomy works by interrupting the route that sperm take from the testicles (where they are produced) to the penis. After a vasectomy, the testicles still continue to generate sperm, but their movement is blocked.
Vasectomy does not affect a man's ability to perform sexually or his sexual satisfaction. It does not change male hormones, male sex characteristics, the sex drive, or semen production.
Vasectomy Surgery
Vasectomy surgery is a much simpler operation than female sterilization. It usually takes 20 minutes to perform and is done at a surgeon's office or outpatient surgery clinic. Local anesthesia is used and the man can return home the same day. In some states, a consent must be signed at least 30 days prior to vasectomy and re-signed on the day of the procedure.
After Surgery
You will feel sore for a few days, but discomfort can be eased by pain relievers and an ice pack. Normal activities can be resumed within a few weeks. For the first few months after vasectomy, some active sperm are still delivered to the semen so you will need to use birth control until a semen analysis confirms the absence of live sperm.
It takes, on average, about 3 months to clear sperm from the reproductive system. You will have a semen analysis (post-vasectomy semen analysis, PVSA) about 12 weeks after vasectomy to verify that no live sperm remain in the semen. You and your partner should continue to use other methods of birth control until the sperm count is zero.
Vasectomy Reversal
The decision to have a vasectomy should be carefully considered. A reversal procedure can be performed, but it does not guarantee restored fertility. In addition, these reversal procedures (vasovasostomy and vasoepididymostomy) are much more complicated surgeries than vasectomy. Insurance may not cover the cost of vasectomy reversal.
American Urological Association Guidelines
The American Urological Association (AUA) recommends that a man considering a vasectomy should meet with his doctor for a preoperative consultation. The AUA emphasizes that it is important for men to understand that a vasectomy is intended as a permanent form of contraception.
Introduction
Vasectomy is male sterilization. It is a method of permanent birth control for men. A man who has had a successful vasectomy cannot make a woman pregnant.
A vasectomy is surgery to block the vas deferens. These are the 2 tubes that carry sperm from the testicles (where sperm is produced) to the urethra (where sperm is ejaculated). After vasectomy, the testicles still continue to generate sperm, but their movement out of the testicles is blocked. Eventually the sperm die, and the body naturally absorbs them. During sex, semen is produced in the same amount as before vasectomy, but this fluid does not contain sperm.
Vasectomy should not be confused with castration. It does not affect a man's ability to perform sexually, or his sensation of orgasm and pleasure. It does not change male hormones, male sex characteristics, or sex drive. Testosterone continues to be produced in the testes and delivered into the bloodstream. Sperm form a very small portion of semen, so men notice no difference in the amount of semen produced during orgasm.
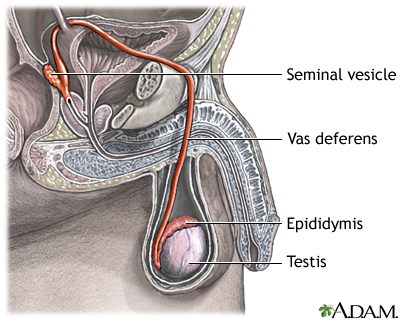
The testicles (testes) are where sperm are produced in the scrotum. The epididymis is a tightly-coiled tube that lies against each testicle and connects ducts from the testicle to the vas deferens. Sperm from the testicles are collected and stored in the epididymis where they begin the process of maturation. When ejaculation occurs, rhythmic muscle movements propel the sperm forward. The sperm are forcefully expelled from the tail of the epididymis into the vas deferens. The vas deferens joins with the seminal vesicle to form the ejaculatory duct, which passes through the prostate and empties into the urethra.
The Male Reproductive System
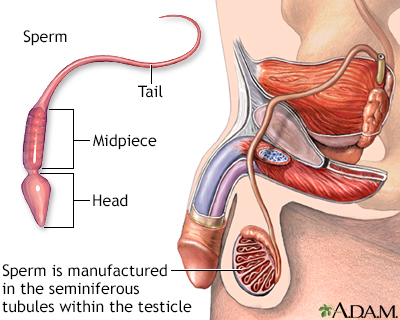
Sperm and Ejaculation
The sperm's journey through the male body is long and complex:
- Sperm are produced in the testes (testicles) within tiny ducts called seminiferous tubules.
- Sperm in each testicle pass into a tightly coiled structure called the epididymis. Sperm mature in the epididymis and are held here until sexual activity forces them to move on.
- When a man experiences sexual excitement, nerves stimulate each epididymis to contract. This forces the sperm to pass into a muscular channel called the vas deferens. (The 2 vas deferens are called the vasa deferentia. Vasectomy blocks both vasa deferentia to interrupt the transport of sperm.)
- Muscle contractions in the vas deferens from sexual activity propel the sperm along past the seminal vesicles, which are glands that contribute seminal fluid (semen) to the sperm. The vas deferens also collects fluid from the nearby prostate gland. Semen is composed mainly of these fluids from the seminal vesicles and prostate. Sperm make up only a small portion of semen.
- Each vas deferens and seminal vesicle then join together to form the ejaculatory duct. This duct, which now contains the sperm-containing semen, opens into the urethra. (The urethra is the same channel in the penis through which a man urinates. During orgasm the bladder neck closes so urine cannot enter the urethra.)
- The semen is forced through the urethra during ejaculation, the final stage of orgasm when the sperm are literally ejected from the penis.
Treatment
After deciding that permanent birth control is the best solution, a couple still has the option of choosing either vasectomy for the male or tubal ligation (female sterilization) for the female. Female sterilization is performed much more often than vasectomy, but vasectomy is a less complicated and less expensive procedure, and poses fewer risks for complications.
Vasectomy is very safe and is nearly 100% effective for preventing pregnancy. It does not protect against sexually transmitted infections (STIs). Condoms remain the best method of STI prevention for sexually active people.
Vasectomy does not affect sexual function or pleasure. It does not noticeably decrease the amount of semen produced during orgasm.
The decision to have a vasectomy should be carefully considered. A reversal procedure can be performed, but it is a major operation that does not guarantee restored fertility. In addition, these reversal procedures (vasovasostomy and vasoepididymostomy) are much more complicated surgeries than vasectomy. While currently in the United States most health insurance plans will cover all or part of the cost of a vasectomy, many insurance plans will not pay for the cost to reverse a vasectomy.
A vasectomy is usually performed by a urologist, a doctor who specializes in the male reproductive system.
Who Should Have a Vasectomy
Vasectomy may be a good choice for a man who:
- Is in a relationship, and both partners agree that they do not want children or additional children. They do not want to use, or cannot use, other methods of contraception.
- Is in a relationship and a pregnancy would be unsafe for the woman partner because of health problems.
- Is in a relationship, and one or both partners have genetic disorders that they do not want to pass on.
- Does not want to be bothered by having to use other forms of birth control during sexual activity.
Vasectomy may not be a good choice for a man who:
- Is in a relationship with someone who has not decided on whether to have children in the future.
- Is in an unstable or stressful relationship.
- Is considering the operation just to please a partner.
- Wants to have children later by storing sperm or by reversing the vasectomy.
- Is young and may want to make a different decision in the future.
- Is single when deciding to have a vasectomy. This includes men who are divorced, widowed, or separated.
- Is unsure whether he should have a vasectomy.
Sperm Banking
In rare cases, a man may choose to use sperm banking before a vasectomy. Sperm banking involves freezing (cryopreservation) and storage (cryobanking) of sperm. If a man later desires to have children, the sperm can be used for assisted reproductive technologies, usually intracytoplasmic sperm injection (ICSI) used in combination with in vitro fertilization.
Sperm banking does not guarantee a successful conception and pregnancy. Sperm can be frozen for many years, but even after several months some sperm cells lose their ability to function normally after being unfrozen. In addition, sperm banking is expensive and is typically not covered by health insurance plans.
Men who are considering vasectomy should not view sperm banking (or vasectomy reversal surgery) as a guaranteed option if they later change their minds. It is best to undertake vasectomy as a permanent sterilization procedure. If future fathering of children seems a possibly desirable scenario, it is wise to reconsider whether vasectomy is the right decision to make.
Vasectomy Surgery
Vasectomy is a minor surgical operation that takes about 20 minutes. It is usually performed with local anesthesia in a doctor's office, outpatient surgery facility, or a family planning clinic.
You will be awake during the procedure but will not feel any pain. If you choose, you can have oral sedation to help you relax.
There are two basic types of vasectomy:
- Conventional vasectomy uses 1 to 2 incisions in the scrotum. The incision is closed with dissolvable sutures.
- No-scalpel vasectomy (NSV) is much more commonly performed. In this minimally invasive procedure, the surgeon makes a tiny hole in the skin of your scrotum by separating the skin with a sharp instrument. No stitches are used. A special glue may be used to seal the skin.
- Both procedures involve cutting and sealing each vas deferens.
Before the Procedure
- Do not take aspirin, ibuprofen (Advil, generic), or naproxen (Aleve, generic) in the week before surgery. These drugs can increase the risk for bleeding. If you need a painkiller, use acetaminophen (Tylenol, generic). If you are taking a blood thinner you may be asked to stop it 5 to 7 days prior to the procedure as long as it is ok with your physician.
- On the day of the vasectomy, shower and shave the hair off your scrotum.
- Wear loose-fitting comfortable pants. Bring along an athletic supporter (jockstrap). You will wear this after the procedure to help reduce swelling.
- If you are having sedation, arrange for someone to pick you up and drive you home.
Before the surgeon starts the procedure, you will receive an injection of local anesthetic into your scrotum and vas deferens. Some surgeons offer "no-needle" NSV, which uses a jet injector to spray the anesthetic.
Conventional Vasectomy
A conventional vasectomy procedure is performed as follows:
- The surgeon makes a small incision on one side of the scrotum and locates one vas deferens. The vas deferens is lifted out through the incision and cut. A section may be removed.
- The surgeon then seals the end of the tube using a heat-generating electric needle (electrocauterization), sutures (ligation), or clamps. Cauterization is usually preferred. Various techniques, such as fascial interposition, may be used along with cauterization to improve the chance of permanent closure.
- The surgeon may choose to close off either one end of the vas (called an open-ended procedure) or both ends (closed-ended technique). In the open-ended procedure, the vas section connected to the testicle is left open, and the one leading to the prostate is sealed. In the closed-ended approach, both are sealed. After closing off the tube, the vas deferens is gently placed back into the scrotum.
- The procedure is then repeated on the other side.

Click on the icon to see an illustrated series detailing a vasectomy.
No-Scalpel Vasectomy
Minimally-invasive techniques are now the preferred methods for vasectomy. The most popular of these, called NSV, has been in use since 1974.
NSV does not require a scalpel or incisions:
- The surgeon uses a hemostat, a sharp surgical instrument to puncture a small hole in the scrotum.
- The opening is gently stretched and the vas deferens is pulled through the hole. The vas is then sealed off using the same methods as conventional vasectomy. As with standard vasectomy, the closures can be open- or closed-ended.
- No stitches are needed to close the tiny opening, which heals quickly and leaves no scar. Sometimes a special glue is used to seal the skin.
Less Common Vasectomy Procedures
The Pro-Vas vasectomy does not involve cutting the vas deferens. Instead, it uses a clip locked around the vas deferens to stop the flow of sperm. To date, there is insufficient evidence that the clip method is superior to other vasectomy methods. Many insurance companies consider this procedure to be experimental and will not pay for it.
Recovery
Vasectomy is a low-risk procedure. Pain or soreness typically lingers for a few days after the procedure, but this is normal.
The following are some tips to help speed recovery:
- The local anesthetic wears off about 1 to 3 hours after the procedure, and you may then experience a dull ache in the testicles and groin. You can take acetaminophen (Tylenol, generic) to cope with the pain. Rest and stay off your feet for 24 to 48 hours. It is best to lie on your back.
- Wear an athletic supporter (jockstrap). You can also reduce swelling by applying an ice pack or bag of frozen peas to your scrotum.
- Avoid any heavy lifting or exercise for several days. You can most likely return to work in a few days if it is not physically demanding.
- Ask your surgeon when you can resume having sex. You must use contraception until a semen analysis confirms that no functional sperm remain.
- The American Urological Association recommends that men refrain from ejaculating for a week following vasectomy.
Semen Analysis
Vasectomy does not produce immediate sterility. After the vasectomy procedure, there are always some active sperm left in the semen for several months, so the risk for pregnancy persists. You are considered sterile if the results of a post-vasectomy semen analysis (PVSA) show that:
- There are no live sperm in your semen (azoospermia)
- There are only rare, not moving sperm (rare non-motile sperm or RNMS). For a vasectomy to be considered successful, RNMS should be less than 100,000/mL semen.
It takes, on average, about 3 months to clear the viable sperm from the reproductive system, but it may take some men as long as 6 months to become sterile. The doctor will perform a semen analysis about 8 to 16 weeks after vasectomy to verify that no live sperm remain in the semen. It is essential that the man and his partner continue to use other methods of birth control until his sperm count is zero. Several semen analyses may be performed to verify that there are no live sperm.
Many men who have vasectomies never bother to return for follow-up sperm testing (semen analysis). Without a follow-up test, men do not know whether the vasectomy was successful. Until test results verify that there are no sperm in the semen, men are at risk of fathering unwanted pregnancies. In addition to a lab test, there is an FDA-approved test kit (SpermCheck Vasectomy), which can be used at home.
If results of a semen analysis do not indicate sterility 6 months after vasectomy, the procedure may be considered a failure. Repeat vasectomy may be an option. Failed vasectomies are rare, and repeat vasectomies are needed less than 1% of the time.
Pregnancy rates after a successful vasectomy are very low, about 1 in 2,000. There are 2 main reasons for an unexpected pregnancy:
- Residual sperm were still alive when the partners had unprotected sex. This is the most common reason for an unexpected pregnancy after a vasectomy.
- Recanalization may cause vasectomy failure. This is when the cut ends of the vas grow back together.
- If sperm still appear in your semen analysis after several months, recanalization may be the problem. A repeat vasectomy will be needed in less than 1% of cases.
Complications
Serious complications are rare after vasectomy but can occasionally occur.
Short-term complications after the procedure may include:
- Bleeding. Blood may seep under the skin, so that the scrotum and penis appear to be bruised. If there is no dangerous swelling, this painless and common problem usually disappears without treatment within 1 to 2 weeks. If the bleeding is excessive and requires more than 2 to 3 gauze changes per day, contact your health care provider. If blood collects in the scrotum, the scrotum can swell up and be firm or tender. This is called a hematoma. Most of the time this will resolve on its own but may take several weeks. You should notify your surgeon if this happens.
- Infection. The incision site may become infected, causing redness and swelling around the incision. Antibiotics will usually clear the infection in a few days.
Long-term complications are very rare but may include:
- Recanalization. This is when the cut ends of the vas deferens reconnect. Recanalization can occur in months, or in rare cases years, after vasectomy.
- Sperm granulomas are tiny hard nodules that develop from sperm leaking out of the vas deferens. Granulomas usually go away on their own, but can cause pain. They can be treated with pain medication. Sometimes surgery may be needed to remove a granuloma.
- Epididymitis. This is an inflammation or infection of the epididymis, the coiled structure on the testicle where sperm are stored. This rare condition usually occurs within the first year and is treated with antibiotics, pain relievers, and heat or cold therapy. An open-ended vasectomy may reduce the risk for this complication.
- Testicular pain (or orchialgia) develops in some men. If this pain lasts longer than 3 months, it is called post-vasectomy pain syndrome (PVPS). The causes of PVPS are unclear. PVPS is first treated conservatively, with heat or cold therapy, rest, scrotal support, and pain relievers. If these methods do not work, other drug therapies (including injections of local anesthetics or steroids) may be tried. Transcutaneous electrical nerve stimulation (TENS) is another treatment. As a last resort, surgical interventions, including vasectomy reversal, may be required. Anewer technique called micro-denervation of the spermatic cord (MDSC) is currently being evaluated as therapy for PVPS.
- Prostate cancer has been raised as a possible long-term complication. Most recent data does not support an association between either vasectomy or vasectomy reversal and prostate cancer risk. There does not need to be any change in choices for screening for prostate cancer based on history of having a vasectomy.
Reversal Surgery (Vasovasostomy and Vasoepididymostomy)
Although men should consider vasectomy a permanent decision, reversal procedures can restore fertility in some men who change their minds. Vasectomy reversal is also sometimes performed to provide pain relief for men who experience persistent post-vasectomy pain in their testicles.
Vasovasostomy Reversal Surgery Procedures
There are two types of vasectomy reversal surgical procedures:
- Vasovasostomy. The cut ends of the vas deferens are sewn back together.
- Vasoepididymostomy. The vas deferens is surgically reattached directly to the epididymis. This procedure is more difficult to perform and is used when vasovasostomy cannot be performed or does not work.
These procedures help restore sperm flow so that sperm can be ejaculated out of the urethra. Both types of procedures are generally performed on an outpatient basis, and the man can return home the same day.
It is not possible to know in advance which procedure will be performed. The surgeon will make the decision whether to use vasovasostomy or vasoepididymostomy based on a fluid sample taken at the start of the operation. The fluid is removed from the vas end closest to the testicle and examined for its appearance and the presence of sperm:
- If sperm is present or the fluid is clear, it indicates that there is no blockage in the epididymis, and a vasovasostomy can be performed.
- No sperm, or a creamy, thick appearance of fluid, is a sign of blockage, and the vasoepididymostomy surgical approach to bypass the blockage should be used.
- Other factors may also determine the surgeon's choice of reversal surgical procedure. In some cases, a combination of the two surgeries may be used.
Vasovasostomy uses several different surgical approaches. Usually a microsurgical technique is used, in which a microscope helps magnify the surgical area. Vasovasostomy takes 2 to 3 hours to perform. The man is given local anesthesia and a mild sedative. Some surgeons may prefer this to be done under general or spinal anesthesia.
Vasoepididymostomy is a more complex procedure due to the extremely tiny size of the tubes inside the epididymis. Microsurgical techniques and an experienced surgeon are critical for the success of this procedure. Vasoepididymostomy takes up to 5 hours to perform. The man is given either general anesthesia or an epidural block.
Recovery and Follow-Up
Pain after reversal surgery is usually not severe and can be controlled with acetaminophen (Tylenol, generic). A cold pack placed on the scrotum area can help relieve swelling. Your doctor may recommend that you wear a jockstrap for a few weeks to help provide compression and to keep the surgical incisions in place.
Most men can return to work and resume normal non-strenuous activities within a week, but may need to refrain from heavy lifting and other physical exertion for up to 4 weeks following surgery. Men need to wait several weeks before having sex.
The doctor will perform a semen analysis every 2 to 3 months after reversal surgery to check your sperm count. It generally takes about 2 months for sperm to reappear following vasovasostomy, and about 3 to 15 months following vasoepididymostomy. Either a stabilized sperm count, or pregnancy, indicates successful reversal surgery.
If reversal surgery is not successful, a repeat surgery can be performed. However, the success rates for repeat reversals are lower than for an initial reversal.
Pregnancy Results after Reversal Surgery
Success rates for vasectomy reversal vary, but are usually about 50%. It can take up to 1 to 2 years after reversal surgery for pregnancy to occur.
The time interval between the original vasectomy and the reversal procedure is the most important factor. The shorter the time between vasectomy and reversal, the better the chances for fertility recovery.
Resources
- Planned Parenthood -- www.plannedparenthood.org
- American Urological Association -- www.auanet.org
- Urology Care Foundation -- www.urologyhealth.org
- Vasectomy.com -- www.vasectomy.com
References
Bhindi B, Wallis CJD, Nayan M, et al. The Association Between Vasectomy and Prostate Cancer: A Systematic Review and Meta-analysis. JAMA Intern Med. 2017;177(9):1273-1286. PMID: 28715534 pubmed.ncbi.nlm.nih.gov/28715534.
Cook LA, Van Vliet H, Lopez LM, Pun A, Gallo MF. Vasectomy occlusion techniques for male sterilization. Cochrane Database Syst Rev. 2014;(3):CD003991. PMID: 24683020 pubmed.ncbi.nlm.nih.gov/24683020.
Handelsman DJ. Male contraception. In: Jameson JL, De Groot LJ, de Kretser DM, et al, eds. Endocrinology: Adult and Pediatric. 7th ed. Philadelphia, PA: Elsevier Saunders; 2016:chap 142.
Hawksworth DJ, Khera M, Herati AS. Surgery of the scrotum and seminal vesicles. In: Partin AW, Dmochowski RR, Kavoussi LR, Peters CA, eds. Campbell-Walsh Urology. 12th ed. Philadelphia, PA: Elsevier; 2021:chap 83.
Kirby EW, Hockenberry M, Lipshultz LI. Vasectomy reversal: decision making and technical innovations. Transl Androl Urol. 2017;6(4):753-760. PMID: 28904908 pubmed.ncbi.nlm.nih.gov/28904908.
Namekawa T, Imamoto T, Kato M, Komiya A, Ichikawa T. Vasovasostomy and vasoepididymostomy: Review of the procedures, outcomes, and predictors of patency and pregnancy over the last decade. Reprod Med Biol. 2018;17(4):343-355. PMID: 30377390 pubmed.ncbi.nlm.nih.gov/30377390.
Randall S, Boyd J, Fuller E, et al. The Effect of Vasectomy Reversal on Prostate Cancer Risk: International Meta-Analysis of 684,660 Vasectomized Men. J Urol. 2018;200(1):121-125. PMID: 29524505 pubmed.ncbi.nlm.nih.gov/29524505.
Sharlip ID, Belker AM, Honig S, et al. Vasectomy: AUA guideline. J Urol. 2012;188(6 Suppl):2482-2491. PMID: 23098786 pubmed.ncbi.nlm.nih.gov/23098786.
Sinha V, Ramasamy R. Post-vasectomy pain syndrome: diagnosis, management and treatment options. Transl Androl Urol. 2017;6(Suppl 1):S44-S47. PMID: 28725617 pubmed.ncbi.nlm.nih.gov/28725617.
Smith-Harrison LI, Smith RP. Vasectomy reversal for post-vasectomy pain syndrome. Transl Androl Urol. 2017;6(Suppl 1):S10-S13. PMID: 28725612 pubmed.ncbi.nlm.nih.gov/28725612.
Tan WP, Levine LA. Micro-denervation of the spermatic cord for post-vasectomy pain management. Sex Med Rev. 2017;S2050-0521(17)30066-5. PMID: 28735684 pubmed.ncbi.nlm.nih.gov/28735684.
Wilson CL. Vasectomy. In: Fowler GC, ed. Pfenninger and Fowler's Procedures for Primary Care. 4th ed. Philadelphia, PA: Elsevier; 2020:chap 111.
Review Date: 2/27/2020
Reviewed By: Sovrin M. Shah, MD, Assistant Professor, Department of Urology, The Icahn School of Medicine at Mount Sinai, New York, NY. Review provided by VeriMed Healthcare Network. Also reviewed by David Zieve, MD, MHA, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.
 All rights reserved.
All rights reserved.