| ||||||||||||||||||||||||||||||||||||||||
 |
Your doctor may suggest a c-section when a vaginal birth isn't possible or safe for you or your baby. Many situations can warrant a c-section, and nearly one in four babies in the United States is delivered this way.
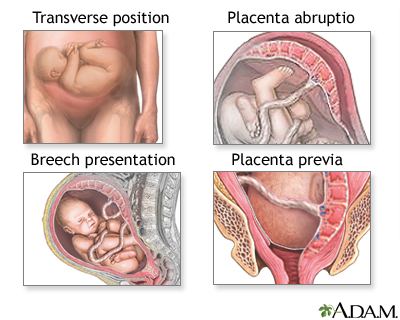
The Following Situations May Make A Vaginal Birth Risky For The Baby:
Other Complications Can Make A Vaginal Birth Risky For The Mother:
Some c-sections are scheduled well in advance, but most are the result of complications that arise during labor. Only a small portion of these is considered "emergency" c-sections - that is, are done to save the mother or baby's life.
If an emergency c-section is needed, your doctor may use general anesthesia, which takes effect almost immediately and renders you unconscious.
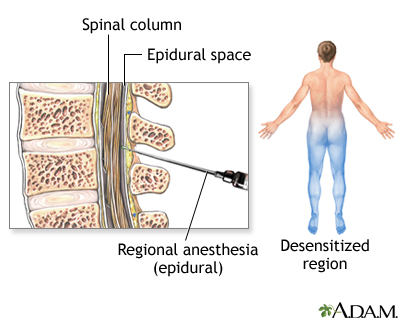
If the c-section is planned or your doctor has a little more time, you'll get a regional anesthetic (such as a spinal or an epidural) that numbs the lower half of your body but leaves you awake and alert.
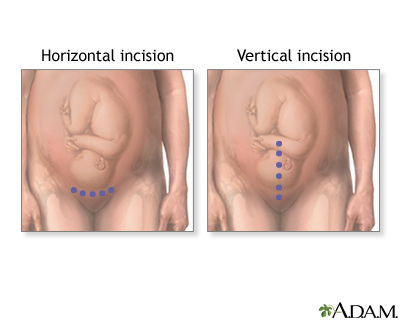
After the anesthesia takes effect, the doctor makes an incision through your abdomen. In most cases, a "bikini cut" is used. This is a horizontal incision just above the pubic area. In an emergency, she may make a vertical cut, which extends from the pubic area to the navel and allows quicker access to the baby.
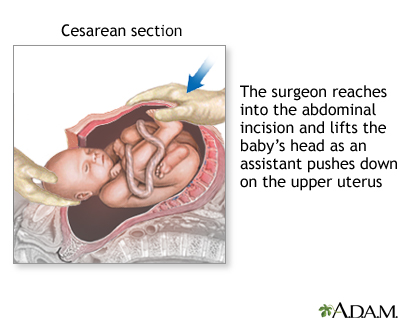
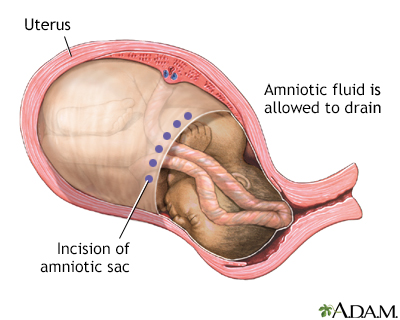
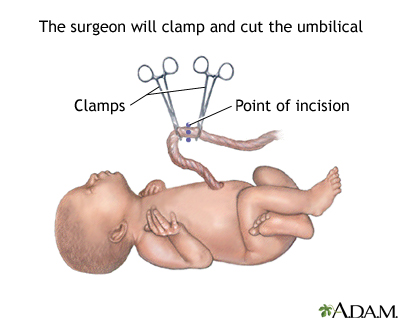
Next, the doctor makes an incision in the uterus (again, either a horizontal or a vertical cut, depending on the situation), suctions out the amniotic fluid, and gently pulls the baby out. While the doctor cuts and clamps the umbilical cord, an assistant suctions mucus from the baby's nose and mouth and makes sure he's breathing well.
After the baby is delivered, the doctor removes the placenta and closes the uterus with dissolvable stitches. She then uses dissolvable stitches or surgical staples (which are removed after about four days) to close the incision in your abdomen.

Once the surgery is done you'll be moved to a recovery room, where nurses will monitor your condition closely for a few hours. As soon as the anesthesia wears off, your doctor will encourage you to get up and walk around, which reduces the risk of a dangerous blood clot (pulmonary embolism) forming.
If you and your baby are both doing well, you'll be discharged from the hospital in two to four days. Recovery from a c-section is often longer and more uncomfortable than recovery from a vaginal birth, so you'll need to get plenty of rest and avoid driving and lifting objects heavier than about 10 pounds until your incision is healed. This includes lifting your other children. You should make plans for having other people take care of your children during the six weeks you are healing.
A cesarean section is major surgery. Risks include an adverse reaction to anesthesia; internal bleeding; blood clots; injury to abdominal organs; and bladder, kidney, or uterine infection. You also may need to have a c-section for future deliveries. (See VBAC (vaginal birth after cesarean)).
Q: How soon after the surgery can I see my baby?
A: If your baby is in good shape, you should be able to see him right away. If there are complications, though, he may need to go to the newborn nursery until his condition is stabilized. Before you head into the operating room, let your doctor know that you'd like to see your baby as soon as possible after the delivery.
Q: Will I need a c-section for my next baby, too?
A: It depends. Since the conditions that lead to c-sections rarely happen in subsequent pregnancies, up to 80% of women can have a trial of labor after cesarean (TOLAC). The exceptions to this rule are women who need a cesarean because of a structural defect (such as a small pelvis or abnormally shaped uterus) and women who had a vertical uterine incision, which is ore likely to rupture during labor. The odds that a regular, horizontal uterine incision will rupture during a TOLAC are very small (1%).
Ultimately, you will need to make a decision with your care provider about whether to try to labor with your next pregnancy.
Q: Can my partner or support person be with me during the c-section?
A: It depends. If the c-section is planned and you're going to be awake during the surgery, most hospitals will allow your partner to stay with you, although you should be sure to discuss this with your caregiver ahead of time. If you have an emergency c-section, your medical team will need to keep distractions to a minimum, so he'll be asked to wait outside the operating room.
|
Review Date:
12/9/2012 Reviewed By: Irina Burd, MD, PhD, Maternal Fetal Medicine, Johns Hopkins University, Baltimore, MD. Review provided by VeriMed Healthcare Network. |
 All rights reserved.
All rights reserved.



