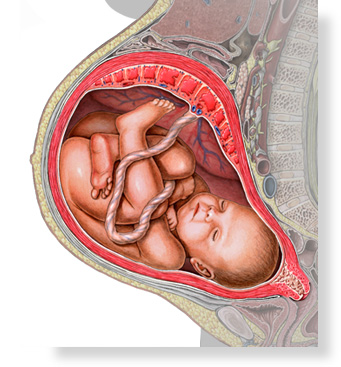
Bleeding and Placenta Problems, Medical Problems, Other Pregnancy Problems
Start here
Preparing for Labor and Delivery, What to Expect During Delivery, Delivery of Your Baby
Start here
Newborn Hospital Care - Routine, Newborn Hospital Care - Sick Child, Going Home With Your Baby
Start here All rights reserved.
All rights reserved.
A.D.A.M. content is best viewed in IE9 or above, Firefox and Google Chrome browsers.