Nuclear stress test
Sestamibi stress test; MIBI stress test; Myocardial perfusion scintigraphy; Dobutamine stress test; Persantine stress test; Thallium stress test; Stress test - nuclear; Adenosine stress test; Regadenoson stress test; CAD - nuclear stress; Coronary artery disease - nuclear stress; Angina - nuclear stress; Chest pain - nuclear stress
Nuclear stress test is an imaging method that uses radioactive material to show how well blood flows into the heart muscle, both at rest and during activity.
Images
How the Test is Performed
This test is done at a medical center or health care provider's office. It is done in stages:
You will have an intravenous (IV) line started.
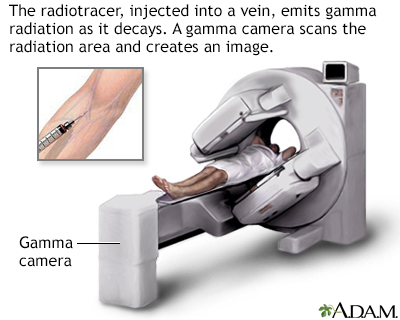
- A radioactive substance, such as thallium or sestamibi, will be injected into one of your veins.
- You will lie down and wait for between 15 and 45 minutes.
- A special camera will scan your heart and create pictures to show how the substance has traveled through your blood and into your heart.
Most people will then walk on a treadmill (or pedal on an exercise machine).
- After the treadmill starts moving slowly, you will be asked to walk (or pedal) faster and on an incline.
- If you are not able to exercise, you may be given a medicine called a vasodilator (such as adenosine or dipyridamole [persantine]). This drug widens (dilates) your heart arteries.
- In other cases, you may get a medicine (dobutamine) that will make your heart beat faster and harder, similar to when you exercise.
Your blood pressure and heart rhythm (ECG) will be monitored throughout the test.
When your heart is working as hard as it can, a radioactive substance is again injected into one of your veins.
- You will wait for 15 to 45 minutes.
- Again, the special camera will scan your heart and create pictures.
- You may be allowed to get up from the table or chair and have a snack or drink.
Your provider will compare the first and second set of pictures using a computer. This can help detect if you have heart disease or if your heart disease is becoming worse.
How to Prepare for the Test
You should wear comfortable clothes and shoes with non-skid soles. You may be asked not to eat or drink after midnight. You will be allowed to have a few sips of water if you need to take medicines.
You will need to avoid caffeine for 24 hours before the test. This includes:
- Tea and coffee
- All sodas, even ones that are labeled caffeine-free
- Chocolates, and certain pain relievers that contain caffeine
Many medicines can interfere with blood test results.
- Your provider will tell you if you need to stop taking any medicines before you have this test.
- Do not stop or change your medicines without talking to your provider first.
How the Test will Feel
During the test, some people feel:
- Chest pain
- Fatigue
- Muscle cramps in the legs or feet
- Shortness of breath
If you are given the vasodilator drug, you may feel a sting as the medicine is injected. This is followed by a feeling of warmth. Some people also have a headache, nausea, and a feeling that their heart is racing.
If you are given medicine to make your heart beat stronger and faster (dobutamine), you may have a headache, nausea, or your heart may pound faster and more strongly.
Rarely, during the test people experience:
- Chest discomfort
- Dizziness
- Palpitations
- Shortness of breath
If any of these symptoms occur during your test, tell the person performing the test right away.
Why the Test is Performed
The test is done to see if your heart muscle is getting enough blood flow and oxygen when it is working hard (under stress).
Your provider may order this test to find out:
- How well a treatment (medicines, angioplasty, or heart surgery) is working.
- If you are at high risk for heart disease or complications.
- If you are planning to start an exercise program or have surgery.
- The cause of new chest pain or worsening angina.
- What you can expect after you have had a heart attack.
The results of a nuclear stress test can help:
- Determine how well your heart is pumping
- Determine the proper treatment for coronary heart disease
- Diagnose coronary artery disease
- See whether your heart is too large
Normal Results
A normal test most often means that you were able to exercise as long as or longer than most people of your age and sex. You also did not have symptoms or changes in blood pressure, your ECG or the images of your heart that caused concern.
A normal result means blood flow through the coronary arteries is probably normal.
The meaning of your test results depends on the reason for the test, your age, and your history of heart and other medical problems.
What Abnormal Results Mean
Abnormal results may be due to:
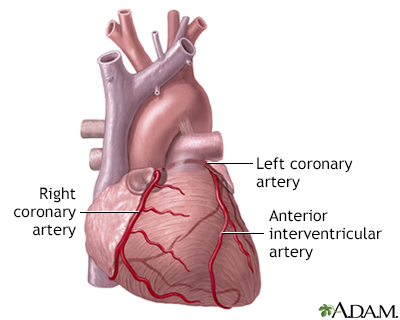
- Reduced blood flow to a part of the heart. The most likely cause is a narrowing or blockage of one or more of the arteries that supply your heart muscle.
- Scarring of the heart muscle due to a previous heart attack.
After the test you may need:
- Angioplasty and stent placement
- Changes in your heart medicines
- Coronary angiography
- Heart bypass surgery
Risks
Complications are rare, but may include:
- Arrhythmias
- Increased angina pain during the test
- Breathing problems or asthma-like reactions
- Extreme swings in blood pressure
- Skin rashes
Your provider will explain the risks before the test.
Considerations
In some cases, other organs and structures can cause false-positive results. However, special steps can be taken to avoid this problem.
You may need additional tests, such as cardiac catheterization, depending on your test results.
Related Information
Exercise stress testChest pain
Heart attack
References
Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64(24):e139-e228. PMID: 25260718 pubmed.ncbi.nlm.nih.gov/25260718/.
Dorbala S, DiCarli MF. Nuclear cardiology. In: Libby P, Bonow RO, Mann DL, Tomaselli GF, Bhatt DL, Solomon SD, eds. Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine. 12th ed. Philadelphia, PA: Elsevier; 2022:chap 18.
Fihn SD, Blankenship JC, Alexander KP, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2014;64(18):1929-1949. PMID: 25077860 pubmed.ncbi.nlm.nih.gov/25077860/.
Flink L, Phillips L. Nuclear cardiology. In: Levine GN, ed. Cardiology Secrets. 6th ed. Philadelphia, PA: Elsevier; 2023:chap 8.
BACK TO TOPReview Date: 10/5/2022
Reviewed By: Thomas S. Metkus, MD, Assistant Professor of Medicine and Surgery, Johns Hopkins University School of Medicine, Baltimore, MD. Also reviewed by David C. Dugdale, MD, Medical Director, Brenda Conaway, Editorial Director, and the A.D.A.M. Editorial team.

Health Content Provider
06/01/2025
|
A.D.A.M., Inc. is accredited by URAC, for Health Content Provider (www.urac.org). URAC's accreditation program is an independent audit to verify that A.D.A.M. follows rigorous standards of quality and accountability. A.D.A.M. is among the first to achieve this important distinction for online health information and services. Learn more about A.D.A.M.'s editorial policy, editorial process and privacy policy. A.D.A.M. is also a founding member of Hi-Ethics. This site complied with the HONcode standard for trustworthy health information from 1995 to 2022, after which HON (Health On the Net, a not-for-profit organization that promoted transparent and reliable health information online) was discontinued. |
The information provided herein should not be used during any medical emergency or for the diagnosis or treatment of any medical condition. A licensed medical professional should be consulted for diagnosis and treatment of any and all medical conditions. Links to other sites are provided for information only -- they do not constitute endorsements of those other sites. © 1997- 2024 A.D.A.M., a business unit of Ebix, Inc. Any duplication or distribution of the information contained herein is strictly prohibited.
 All rights reserved.
All rights reserved.